A middle-age male arrived by private car with chest pain. He immediately became unresponsive, before an ECG could be recorded.
He was resuscitated from ventricular fibrillation and this 12-lead was recorded:
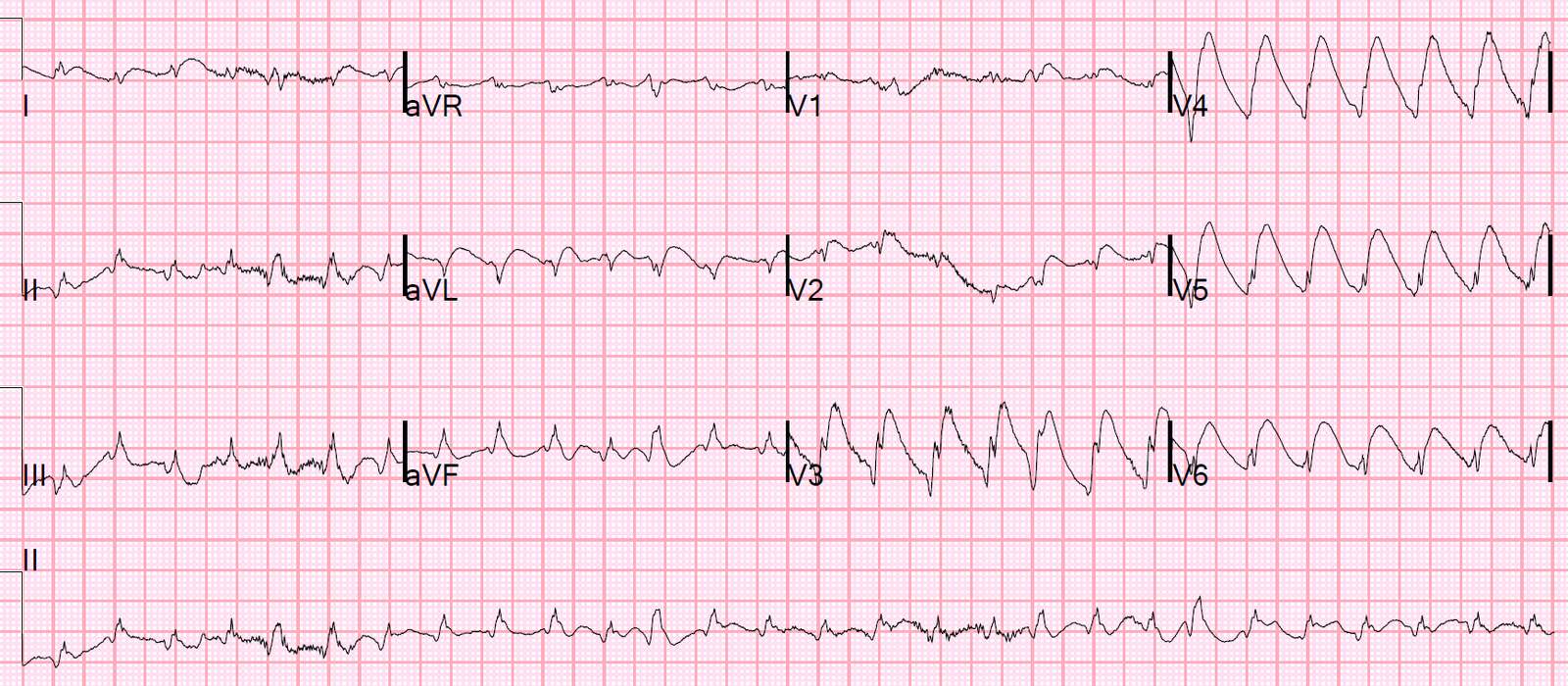 |
| What are the wide complexes in the precordial leads? |
Same ECG with annotation:
 |
| One may perceive these as wide complexes, but they are deceptive. The arrows in V5 and V6 point to narrow complex QRS’s. What appears to be a very wide complex tachycardia is really narrow complex with massive ST elevation and huge hyperacute T-waves. The rate is about 160. The rhythm strip across the bottom (lead II) shows that these relatively normal duration QRS complexes are regular, but with intervening premature ventricular beats (PVC’s, one of which is highlighted by the arrow, complexes 5, 6, 11, 12, 19, 22). Although no P-waves are visible in this, I suspect that it is sinus with PVC’s. PSVT should be converted by a PVC. |
The cath lab was activated and the patient was intubated and received ticagrelor and heparin. There was no treatment of the rhythm, but it gradually slowed down (as one would expect from supportive care in sinus tachycardia).
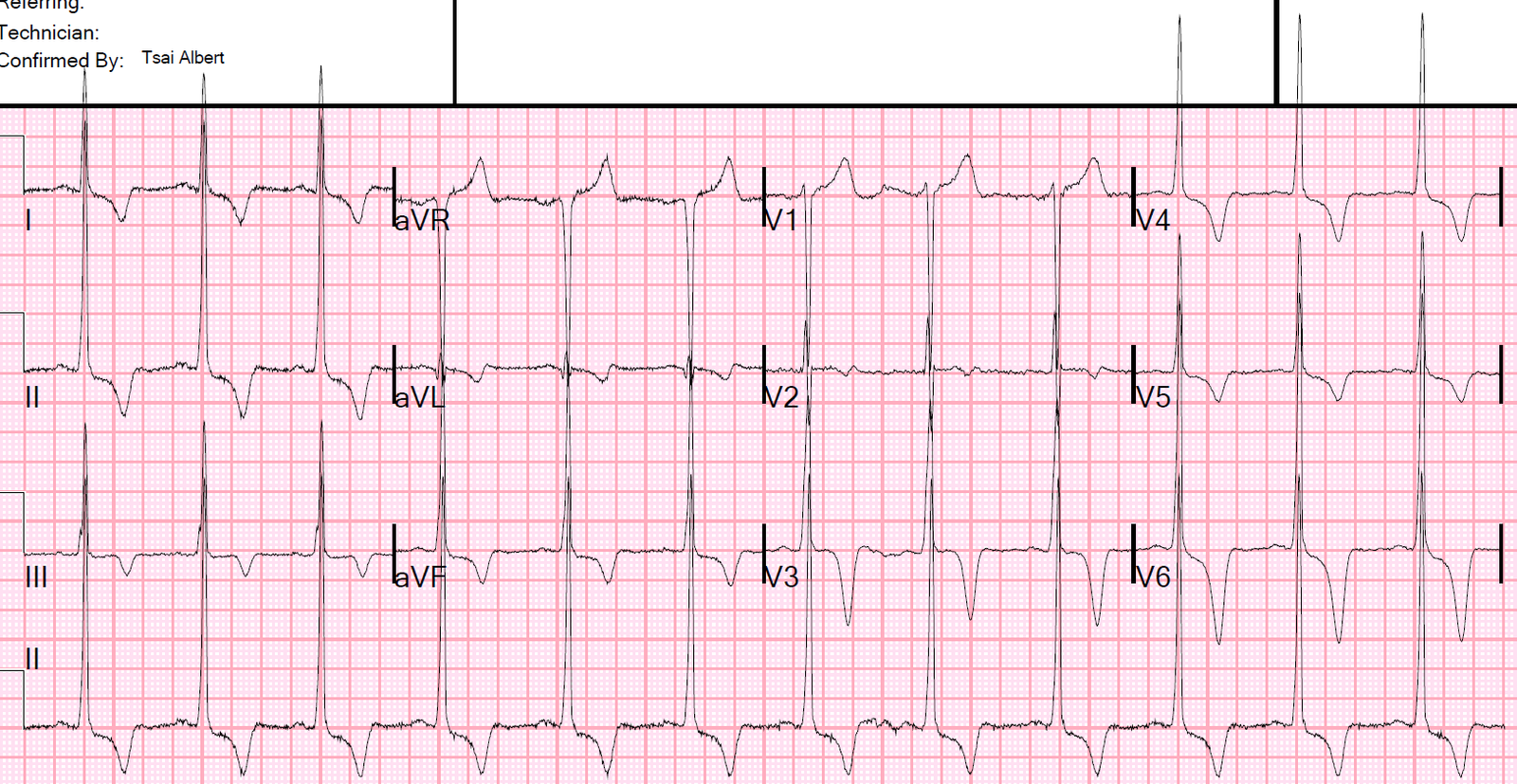
This ECG was recorded just before transportation to the cath lab:
 |
| Sinus tachycardia at a rate of about 100. Massive ST elevation continues. |
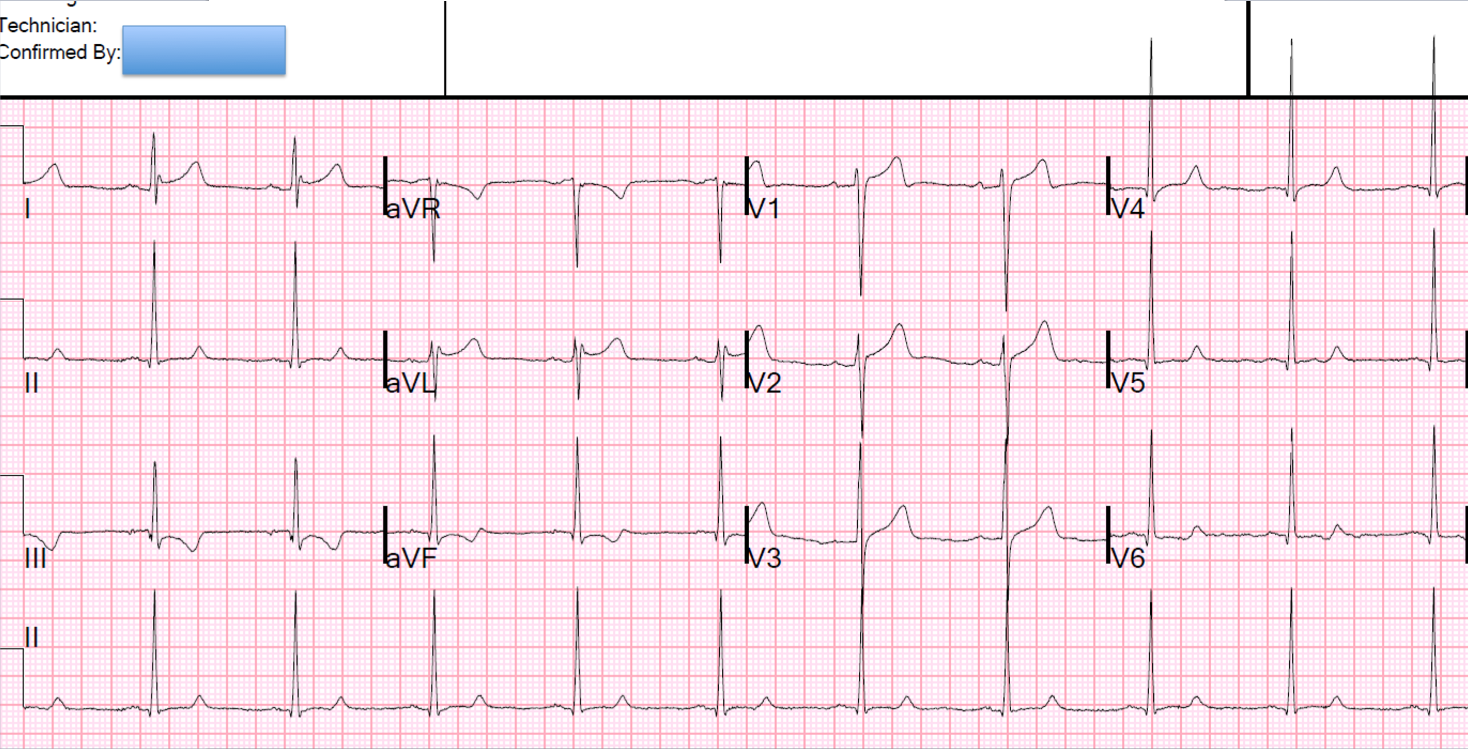
A mid LAD 100% thrombotic occlusion was opened and stented. Door to balloon time was less than 60 minutes. Echo next day showed 57% EF. Peak troponin I was 250 ng/mL.