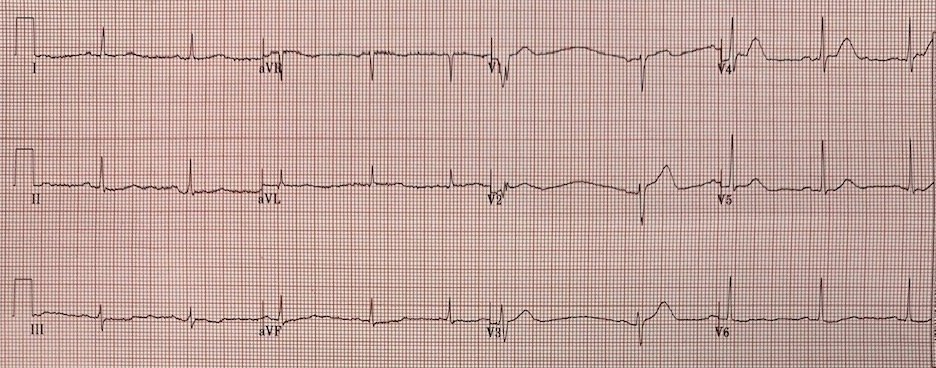
An 18 y.o. female who presented for chest pain. Patient reports productive cough and headache x 4 days. She notes persistent sternal chest pain worse at night and waking her from sleep. She also notes intermittent abdominal pain, describing as a “tightness”.
 |
| “Sinus arrhythmia with variable right bundle origin PVCs”
Is this accurate? |
No.
This is sinus bradycardia with a slightly accelerated right ventricular escape, such that sometimes:
1. the sinus beat is conducted before any ventricular escape (beats 7)
2. the ventricular beat starts at almost the exact same time as the P-wave, and the P-wave therefore does not conduct (beats 6 and 9)
3. the ventricular beat occurs very shortly after the P-wave such that the P-wave does not conduct (beats 2, 3, 5)
4. The ventricular beat fuses to varying degrees with the conducted beat (beats 1, 3, 4, 8)
This is AV dissociation (not NOT AV block).
Her bedside echo was normal and troponins were negative in the ED.
See Dr. Grauer’s extensive discussion below for more detail.
This is not pathologic, and not worrisome.
If you see a patient with such a rhythm, simply walk them around on a monitor to increase the sinus rate. Then the sinus will usurp the ventricular escape and the ECG will normalize at a faster rate. If not, there is then a problem.
The patient was referred for Holter and it was normal.
![]()
===================================
MY Comment by KEN GRAUER, MD (2/20/2020):
===================================
There are LOTS of excellent Learning Points regarding the ECG in this case. For clarity of explanation — I’ve numbered the beats (Figure-1).
- A QUOTE to Remember — As Rosenbaum said, “Every self-respecting rhythm has at least 3 possible explanations”. There are some details about this interesting arrhythmia that I am not certain of. That said — I don’t think anyone can be absolutely certain of these details without additional monitoring.
 |
| Figure-1: The 12-lead ECG and long lead II rhythm strip in this case (See text). |
FIRST — I completely agree with Dr. Smith’s interpretation (given above) — regarding the most important clinical points. I’ll add some additional thoughts.
- For educational purposes — I think the best way to illustrate the Learning Points from this rhythm, is to address the following clinical questions. Please TAKE ANOTHER LOOK at the rhythm in Figure-1, and answer the following:
BASIC Level QUESTIONS:
- Is there AV dissociation?
- Is the P-P interval constant?
- Is there AV block?
- The patient is an 18-year old woman. Is AIVR (ie, an Accelerated IdioVentricular Rhythm) common in this age group?
- WHY do the ventricular beats occur in Figure-1?
- Are there Fusion beats?
- HOW would you define the rhythm in Figure-1?
ADVANCED Level QUESTIONS: These questions are Beyond-the-Core. The answers to them do not alter management of this patient — but I think the answers are insightful, and help to hone your ECG interpretation skills beyond the basic level.
- Are all P waves in the rhythm in Figure-1 the same?
- Is this really a sinus rhythm?
- WHICH are the fusion beats in Figure-1? Do we really know HOW MANY fusion beats there are?
- WHY does QRS morphology of the conducted beats (ie, beats #1,4,7,8) change?
HINT: If you do not use calipers — You will not be able to answer many of the above questions …
Is there AV Dissociation? — By definition, there is transient AV dissociation in Figure-1. That’s because, at least for some brief period of time — there are some P waves that are not related to neighboring QRS complexes!
- I’ve labeled P waves in the long lead II rhythm strip in Figure-2 (BLUE arrows). It looks like beats #1,4,7 and 8 are conducting — because they are all preceded by P waves with a constant and normal PR interval.
- Since the PR interval preceding beats #2,3,5,6 and 9 is clearly much shorter than the PR interval of conducted beats — this means that beats #2,3,5,6 and 9 are not normally conducted. Therefore — there is AV dissociation for these beats!
- For more on AV Dissociation — CLICK HERE.
 |
| Figure-2: P waves in the long lead II rhythm strip have been labeled with BLUE arrows (See text). |
Is the P-P Interval Constant? — Careful observation of the BLUE arrows in Figure-2 should tell you that the P-P interval is not constant. (IF in doubt — calipers will confirm this for you in 2-3 seconds).
- At the least — there is sinus arrhythmia …
Is there AV Block? — There is no evidence of AV block in Figure-2. That’s because although some of the P waves in this rhythm strip are not conducting — P waves never have a chance to conduct, because the PR interval preceding beats #2,3,5,6 and 9 is clearly too short to allow normal conduction.
- PEARL #1 — Remember that there are 3 potential Causes of AV Dissociation: i) AV dissociation due to some form of 2nd or 3rd degree AV Block; ii) AV dissociation by “Usurpation” — in which P waves transiently do not conduct because an accelerated junctional or ventricular rhythm takes over the pacemaking function (because it is faster than the underlying sinus rhythm); and/or, iii) AV dissociation by “Default” — in which a junctional or ventricular escape rhythm takes over by “default” (ie, because of SA node slowing).
Is AIVR Common in an 18yo? — The ventricular beats in Figure-2 are beats #2, 3, 5, 6 and 9. The usual idioventricular escape rate in adults is between 20-40/minute. As per Dr. Smith — since the rate of the ventricular beats in this case is slightly faster than this (ie, ~55-60/minute) — this is a slightly accelerated ventricular rhythm ( = AIVR).
- For brief review of AIVR — CLICK HERE. The common Clinical Settings in which AIVR may occur include: i) as a rhythm during cardiac arrest; ii) in the monitoring phase of acute MI (especially with inferior MI); or, iii) as a reperfusion arrhythmia (following thrombolysis, acute angioplasty, or spontaneous reperfusion). AIVR may also occur in patients with underlying coronary disease, cardiomyopathy, and with digoxin toxicity.
- PEARL #2 — On rare occasions, AIVR may occur intermittently in otherwise healthy subjects without underlying heart disease. In such cases — this rhythm is often associated with increased vagal tone. If these individuals are asymptomatic — the rhythm is generally benign, and no treatment is needed. Assuming the Echo is normal for the 18yo woman in this case — and provided that the “chest pain” reported by this patient is not related to the rhythm we see in Figure-2 — no additional evaluation would be needed.
 |
| Figure-3: I’ve measured R-R intervals in milliseconds in the long lead II rhythm strip (See text). |
WHY do the Ventricular Beats Occur? — To assist in answering this question — I have carefully measured the R-R intervals in the long lead II rhythm strip (Figure-3).
- PEARL #3 — When confronted with a rhythm strip in which there is transient AV dissociation, and you are not certain as to which beat(s) may be conducting — Look for unexpected shortening of the R-R interval. Such shortening usually indicates which beat(s) is being conducted. Conversely — lengthening of the R-R interval often tells you which beat(s) originate from another focus.
- Beat #4 in Figure-3 is preceded by the shortest R-R interval (865 msec) — and we know this beat is conducting.
- The next shortest R-R intervals in Figure-3 precede beats #7 and 8 (1045 msec) — which we know are both conducted by the P waves that precede them.
- The reason all other beats (ie, beats #2,3,5,6 and 9) are at least in part ventricular beats — is that they are all preceded by longer R-R intervals. It is because the appearance of P waves is delayed — that the slightly accelerated ventricular focus “gets tired of waiting”, and puts out a ventricular beat.
Are there Fusion Beats? — To assist in answering this question — I have drawn a Laddergram of the rhythm (Figure-4).
- PEARL #4 — Although becoming comfortable in drawing laddergrams takes time (it literally took me a few decades to get good at this skill!) — learning to read laddergrams is EASY, and takes no more than a few minutes. (IF interested in some user–friendly examples to get you started — CLICK HERE — and HERE — and HERE).
- P waves precede each of the 9 beats in the long lead II rhythm strip in Figure-4. Isn’t it now much easier to see the irregularity in the P-P interval looking at the Atrial (upper level) tier?
- Beats #1,4,7 and 8 are conducting.
- I’ve drawn RED circles at the bottom of the laddergram that represent ventricular origin for beats #2,3,5,6 and 9.
- My educated guess is that the P waves preceding beats #6 and 9 occur too soon before these ventricular beats to be conducted.
- On the other hand — the PR interval preceding beats #2,3 and 5 is a little longer than that preceding beats #6 and 9 — such that there may have been time for some conduction from above to have occurred. Although hard to tell — the QRS of beats #2,3 and 5 appears to be a little smaller and narrower than that for beats #6 and 9 — so beats #2,3 and 5 appear to be Fusion beats (schematically represented in the laddergram by simultaneous conduction into the Ventricular tier from above and below).
- For more on Fusion beats — CLICK HERE.
 |
| Figure-4: Laddergram of the long lead II rhythm strip (See text). |
WHAT is the Rhythm? — The answer to this question leads us to PEARL #5: The term “AV Dissociation” should never be used as a “diagnosis” per se. Instead — optimal rhythm interpretation indicates there is AV dissociation because of which one or two of the 3 potential causes of AV dissociation discussed in PEARL #1 are operative.
- The primary problem in the rhythm shown in Figure-4 is bradycardia. It is because of sinus bradycardia and arrhythmia that AV dissociation is seen, with several beats from a slightly accelerated ventricular focus.
- Thus, the rhythm is not “AV dissociation”. Instead — we see AV dissociation by default of the sinus pacemaker that slows enough to allow the slightly accelerated ventricular focus to put out several ventricular beats. NOTE: Semantically — this is not pure AV dissociation by “default” — since rather than simple ventricular “escape” — the ventricular focus is faster than the 20-40/minute rate of a ventricular escape rhythm.
ANSWERS to the ADVANCED Questions: Earlier — I posed the following Beyond-the-Core questions.
- Are all P waves in the rhythm the same?
- Is this really a sinus rhythm?
- WHICH are the fusion beats in the rhythm? Do we really know HOW MANY fusion beats there are?
- WHY does QRS morphology of the conducted beats (ie, beats #1,4,7,8) change?
 |
| Figure-5: I’ve labeled all P waves with letters (See text). |
My ANSWERS:
- I believe that P wave morphology is not the same for all of the P waves in Figure-5! Although it is true that there will always be some slight “natural” variation in P wave morphology — DON’T YOU THINK that P waves a,c,d and g are clearly more pointed than P waves e,f and i? (I’m not sure about b, which seems to manifest an in-between morphology).
- IF in doubt — GO BACK to the 12-lead tracing in Figure-1, and look at P wave morphology in all 12 leads. I believe there are some subtle differences that are real.
- Note that the rounder P waves (ie, e,f and i) seem to be preceded by a somewhat longer R-R interval. Clinically — I suspect that rather than sinus arrhythmia, this 18yo probably has a wandering atrial pacemaker — with the marked variation in P-P interval (as well as her AIVR) all being manifestations of increased baseline vagal tone. Shift in the site of the atrial pacemaker may be occurring with ongoing variation in vagal tone. That said — to know for certain if the rhythm was a wandering pacer, we’d need a longer period of monitoring — and we’d need to be sure we were seeing at least 3 different P wave morphologies (For more on ECG diagnosis of wandering pacemaker — CLICK HERE).
- Note that we never see a ventricular beat not preceded by any P wave in Figure-5. As a result — we have NO idea as to what a “pure” ventricular beat looks like. It is therefore possible that even beats #6 and 9 might manifest a slight degree of fusion (ie, we have NO idea as to how many fusion beats we are seeing in this rhythm strip).
- Finally — Note that the S wave of the earliest conducted beat (ie, beat #4) is slightly wider than the S wave of conducted beats #7 and 8. I do not think beat #4 is a fusion beat — because the PR interval is identical to that of other conducted beats, and it is only the terminal S wave that looks slightly wider. Instead — earlier occurrence of beat #4 is probably the result of some incomplete RBBB aberration.
BOTTOM LINE — Assuming this 18yo has no underlying structural heart disease — her interesting rhythm is almost certainly benign. There are no acute ST-T wave changes on conducted beats in her 12-lead tracing.
- My hope is that attention to some of the above “picky” details in complex rhythm interpretation are insightful.
Our THANKS to Dr. Smith for presenting this case!
![]()