A 40-something presented with palpitations and had a regular pulse at 170.
Here is his 12-lead ECG:
 |
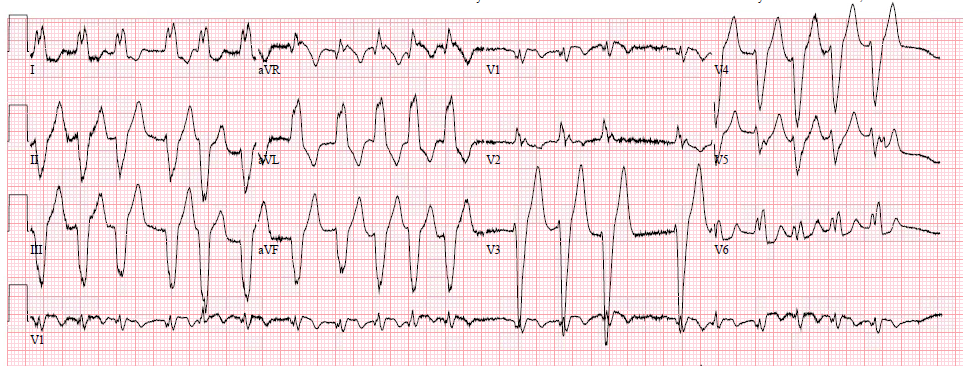
| The computer reads supraventricular tachycardia. What is it? |
It is atrial flutter with 2:1 conduction. It is not PSVT and not sinus.
There are clear flutter waves in lead II across the bottom. In V1, there are upright waves that appear to be P-waves but are not: they are atrial waves and it is typical for atrial flutter waves to be upright in V1, whereas sinus P-waves are biphasic in V1.
The flutter rate is relatively fast at 334, such that the ventricular rate is 167 (one half the atrial rate).
As easy as it may seem to make this diagnosis, it is often misdiagnosed as PSVT. Thus, adenosine is often given.
Such was the case here.
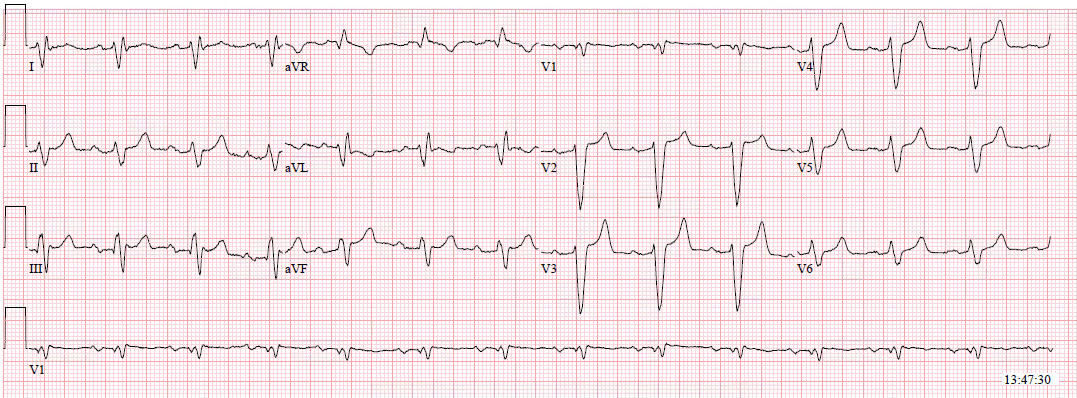
Adenosine was given, during which this rhythm strip was recorded:
 |
| The AV node is blocked by adenosine and QRSs disappear. This “reveals” the flutter waves, which of course continue. There are some ventricular escape beats. |
Adenosine simply blocks the AV node so that there is no QRS to hide the flutter waves, and they become obvious. So adenosine can help to diagnose atrial flutter, but it will not treat atrial flutter.
Atrial flutter does not use the AV node for part of its re-entrant loop, as does PSVT [whether AVNRT (a micro-reentrant intranodal loop) or AVRT (a macro re-entrant loop using bypass tract for one leg of the loop)]. Therefore adenosine will not interrupt the loop.
The half-life of adenosine is about 10 seconds, and its effect will rapidly wear off (thankfully, otherwise this patient would be dependent on ventricular escape beats for perfusion!)
When the adenosine wears off, the impulse will continue to conduct through the AV node, still at a 2:1.
So atrial flutter must be treated with either:
1) A longer acting AV nodal blocker, such as diltiazem infusion, to slow the ventricular response or
2) Cardioversion, whether electrical or chemical. Electrical works better (see article summary at bottom) but has a risk of thromboembolism:
Similarly to atrial fibrillation, patients with atrial flutter do develop atrial thrombi, and thus cardioversion may involve a risk of thromboembolism if the onset of atrial flutter is not within 12-48 hours of ED presentation. This is primarily because patients with atrial flutter often alternate between fib and flutter, and produce thrombi during episodes of fibrillation.
More cases of misdiagnosed atrial flutter
Here are a couple other cases of atrial flutter which were misdiagnosed. In these cases, they were misdiagnosed as sinus tachycardia (not PSVT):
 |
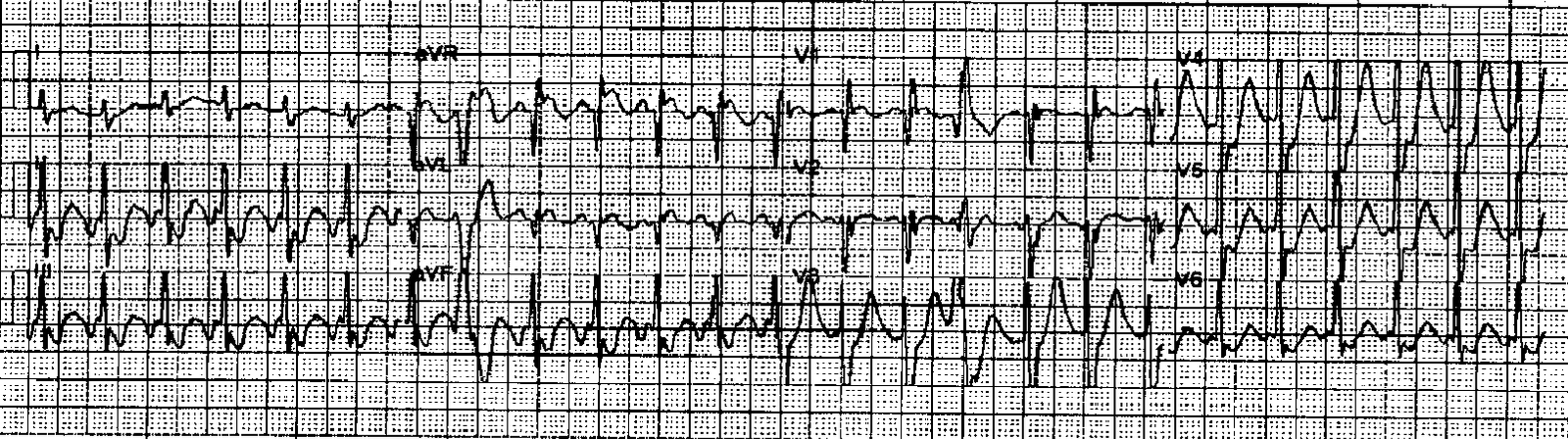
| Notice there is a “P-wave” just before the QRS in V1 Notice there is a “P-wave” directly superimposed (on top of) the T-wave in V1. These are atrial flutter waves. |
 |
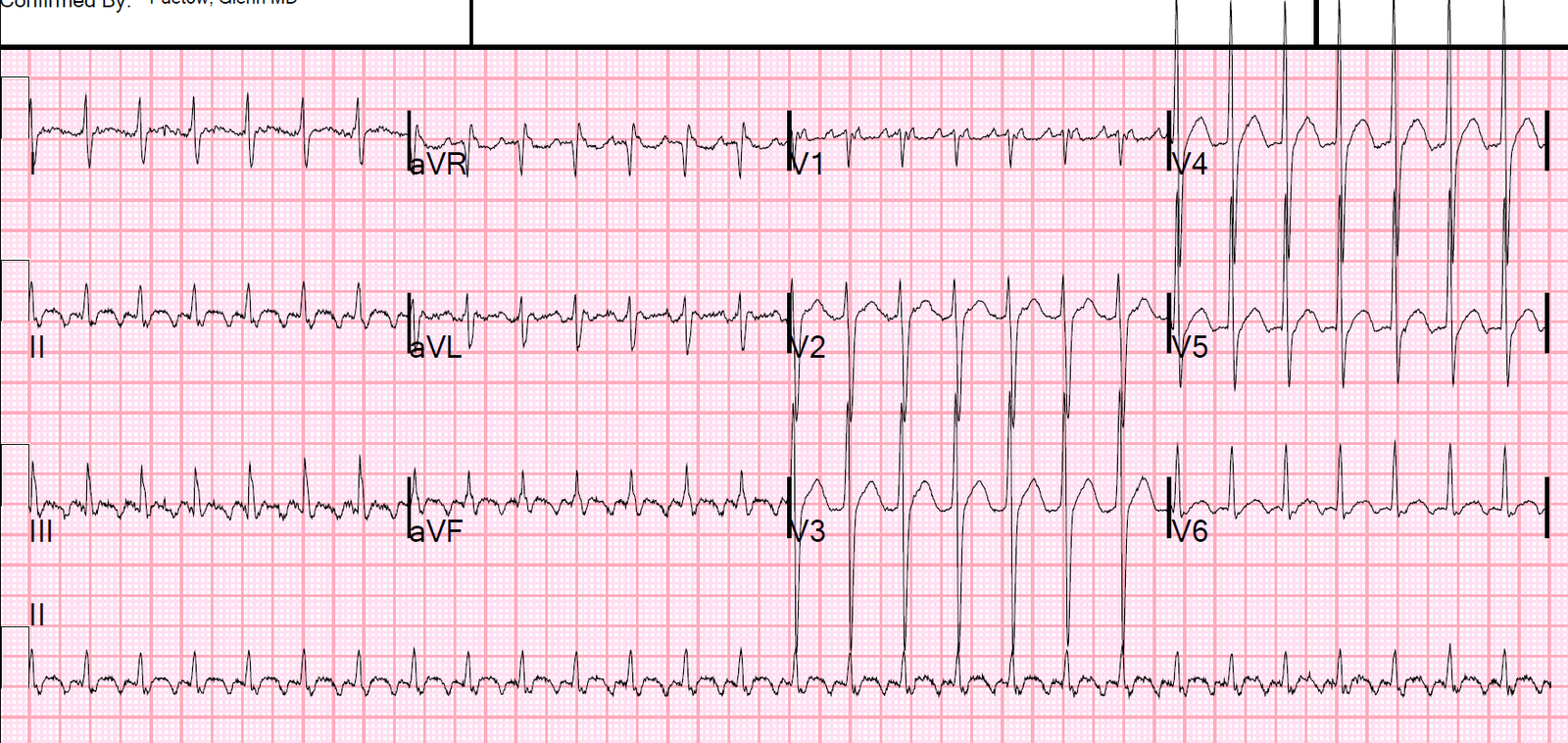
| Narrow complex tachycardia at rate of 135. Notice the “P-waves” are upright in V1 The rhythm strip across the bottom is V1 (it is usually lead II) Notice there is an extra “P-wave” at the end of each QRS in V1 All these are atrial flutter waves. True P-waves are not upright in V1; they are biphasic up-down. The positive deflection of a normal P-wave in V1 is the right atrium The subsequent negative deflection of the normal P-wave in V1 is the left atrium. Thus the flutter rate is 270 with 2:1 conduction. |
 |
| Slow atrial flutter (flutter rate 240, ventricular rate 120) Misdiagnosed as sinus tach Here is the case: Sepsis with Pulmonary Edema and Elevated Right Sided Pressures |
Atrial Flutter rate:
Atrial flutter is usually at a rate of 300, but can be anywhere between 240 and 360.
The ventricular rate depends on AV node conduction and is usually half the atrial rate (2:1 conduction), but may become 1:1 (dangerous) or slow down to less than 2:1 in the presence of AV node blockers
The atrial rate can be much slower in the setting of a sodium channel blocker such as flecainide, quinidine, or procainamide. Use of these medications without prior AV blockade is dangerous as it will lead to 1:1 conduction!!
Atrial Flutter
–Macro re-entrant loop just above AV Node in right atrium
–Atrial rate 240-360 without medications
–2:1 block, vent rate 150 most common
–Regular, fixed; or regularly irregular: RR interval an integer multiple of the atrial rate
–Narrow if no aberrancy or bundle branch block
–Flutter waves, sawtooth pattern–Nearly always visible in lead II
–Adenosine can help to diagnose, not treat
–Conversion vs. Ventricular slowing
l50 Joules, Ibutilide/Amiodarone
lDiltiazem slows at AV node
Procainamide before Diltiazem is dangerous
—it will slow the atrial rate and allow for 1:1 conduction
—results in a FASTER ventricular rate
See this case:
Wide complex tachycardia at a rate of 270
Relevant literature
Emergency Department Management and 1-Year Outcomes of Patients With Atrial Flutter Scheuermayer FX, et al. Annals of EM 57(6):564-571, June 2011
–122 consecutive patients with a primary ED diagnosis of atrial flutter
–1 year: 3 deaths due to concurrent illnesses and no strokes
–Electrical cardioversion resulted in NSR in 91% (42 of 46)
–8 required > 150 Joules
–93% discharged home
–Antiarrhythmic treatment resulted in NSR in 27%
–60% discharged home.
–Same stroke precautions as atrial fib