Case written and submitted by Elzada Sercus M.D., peer reviewed by Pendell Meyers, Steve Smith, and Ken Grauer
A 31-year-old female with a history of low
blood pressure and episodes of lightheadedness developed near syncope on
postpartum day one after an uncomplicated c-section. She has no other past
medical history and does not take any medications. She has no family history of
sudden cardiac death or premature coronary artery disease. Given the patient’s
near syncope, an ECG was obtained and when the patient was placed on continuous
telemetry monitoring was found to have frequent PVCs. She did not experience any
palpitations or sensation of heart racing during the episodes recorded.
She was not having any chest pain at the time the ECG was performed or at any
point preceding or during her near syncopal episodes.
Telemetry monitoring showed sinus rhythm with occasional bradycardia in the 40s-60s, as well as frequent PVCs. Blood pressure ranges were 98-113 mmHg systolic and 82-68 mmHg
diastolic which were baseline for this patient. Potassium was 3.5 mmol/L and
magnesium 1.6 mg/dL, otherwise all laboratory studies were within normal
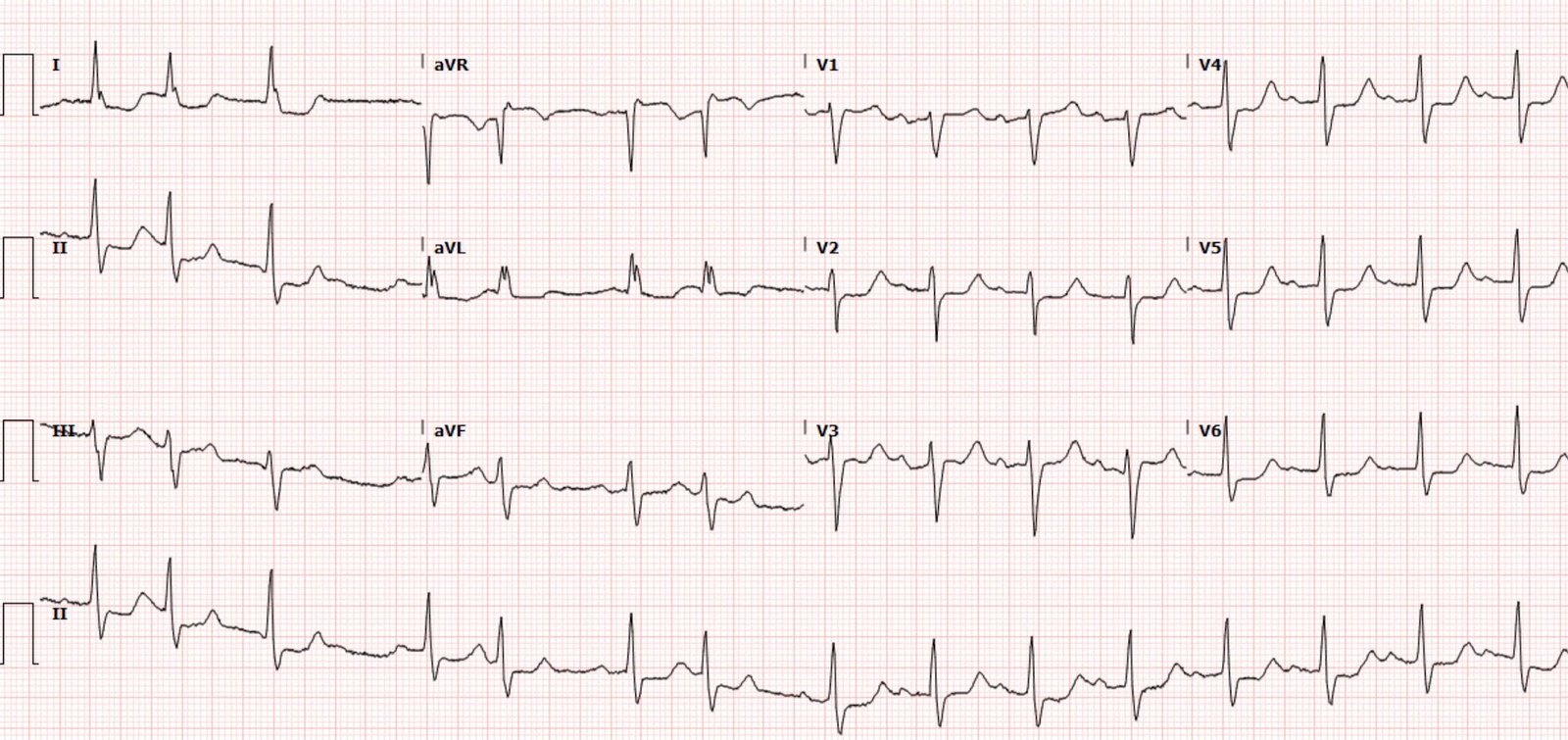
limits. Electrolyte repletion was ordered, and the ECG below was obtained:
 |
| What do you think? What is the rhythm? Is there any evidence of AV block? |
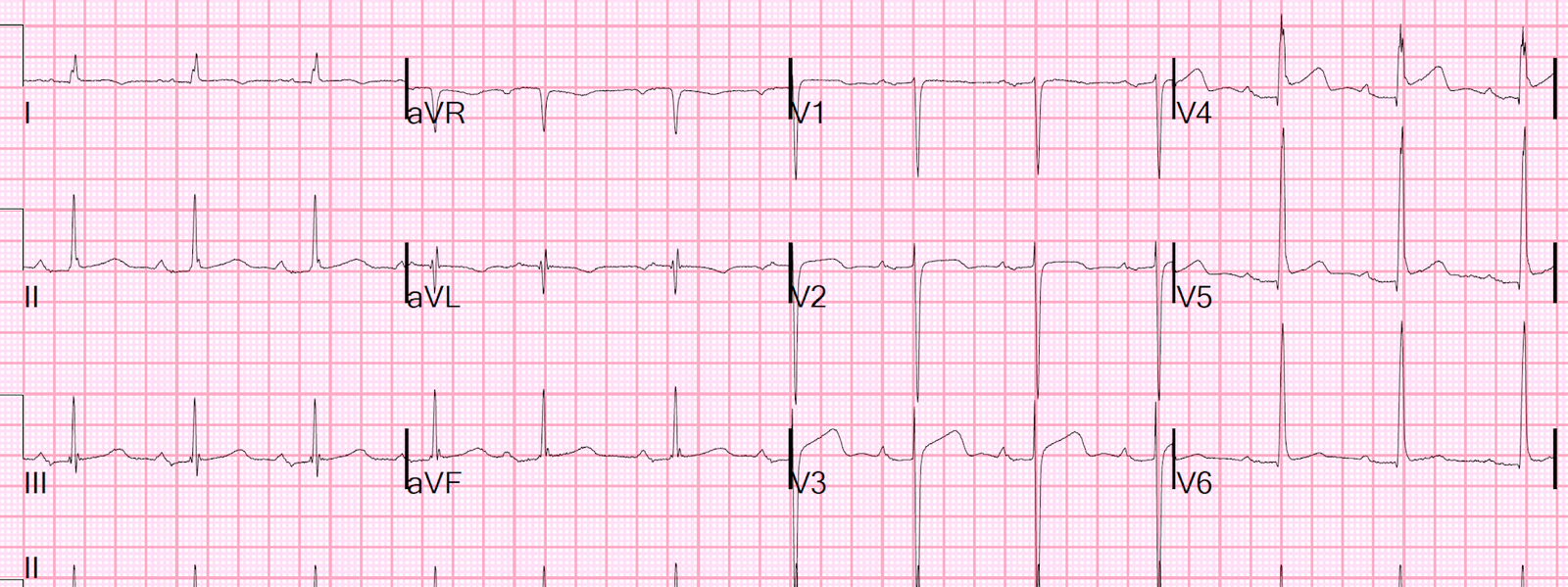
Baseline ECG (taken 5 months prior):

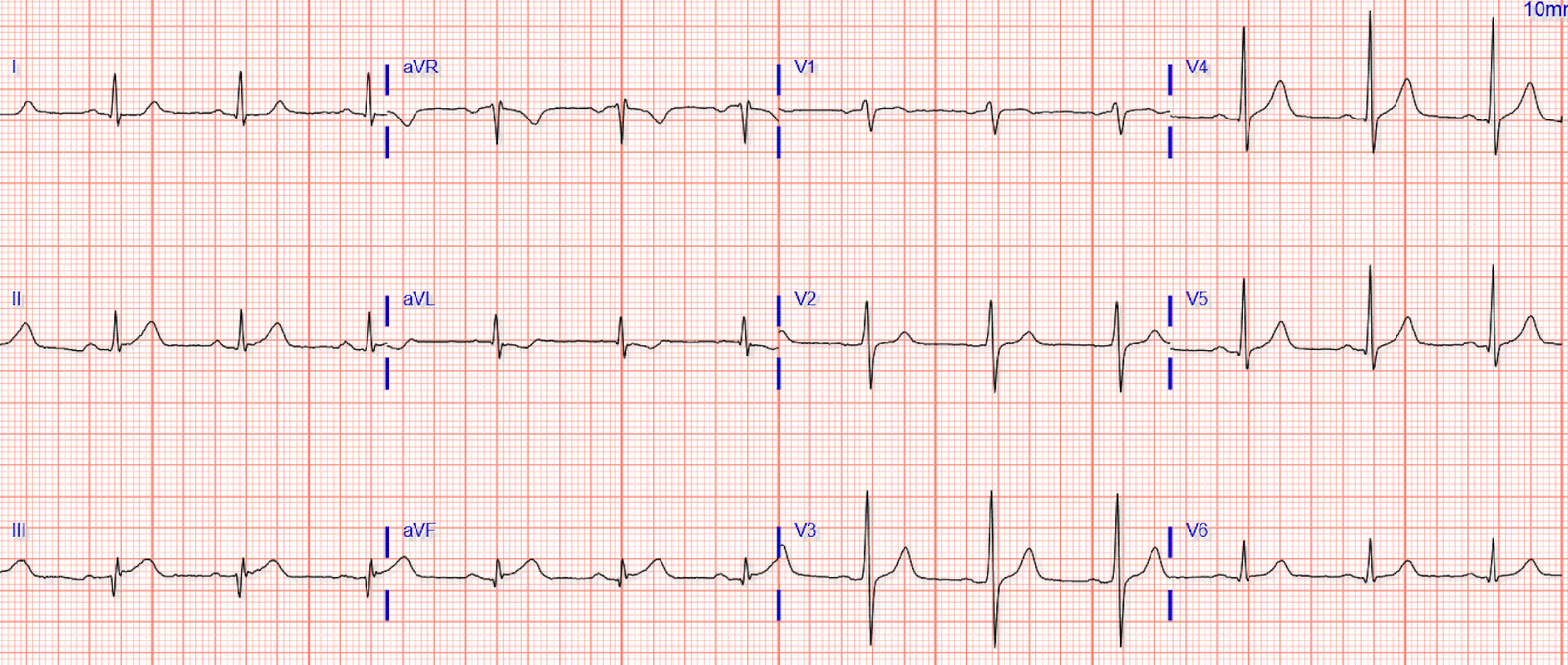
Presentation ECG annotated:
 |
ECG Interpretation:
Normal sinus rhythm (each QRS complex is preceded by a P wave) with frequent unifocal PVCs. There are normally conducted sinus beats (blue arrow) followed by PVCs (green arrow). Following the QRS there appears to be another atrial wave (red arrow) superimposed on the PVC’s T wave, followed then by another narrow complex QRS with slightly different morphology than the normally conducted QRS (after the blue arrow).
At first glance, it may appear that the atrial waves at the red arrow are different than those at the blue arrow. However, closer inspection reveals that they march out perfectly, and when considering the morphology of the ST segment and T wave without a superimposed P wave, these atrial waves are actually both upright and similar (probably identical). They are not inverted, and therefore not retrograde. Thus, the P waves are all sinus, throughout, without fail or change in rate.
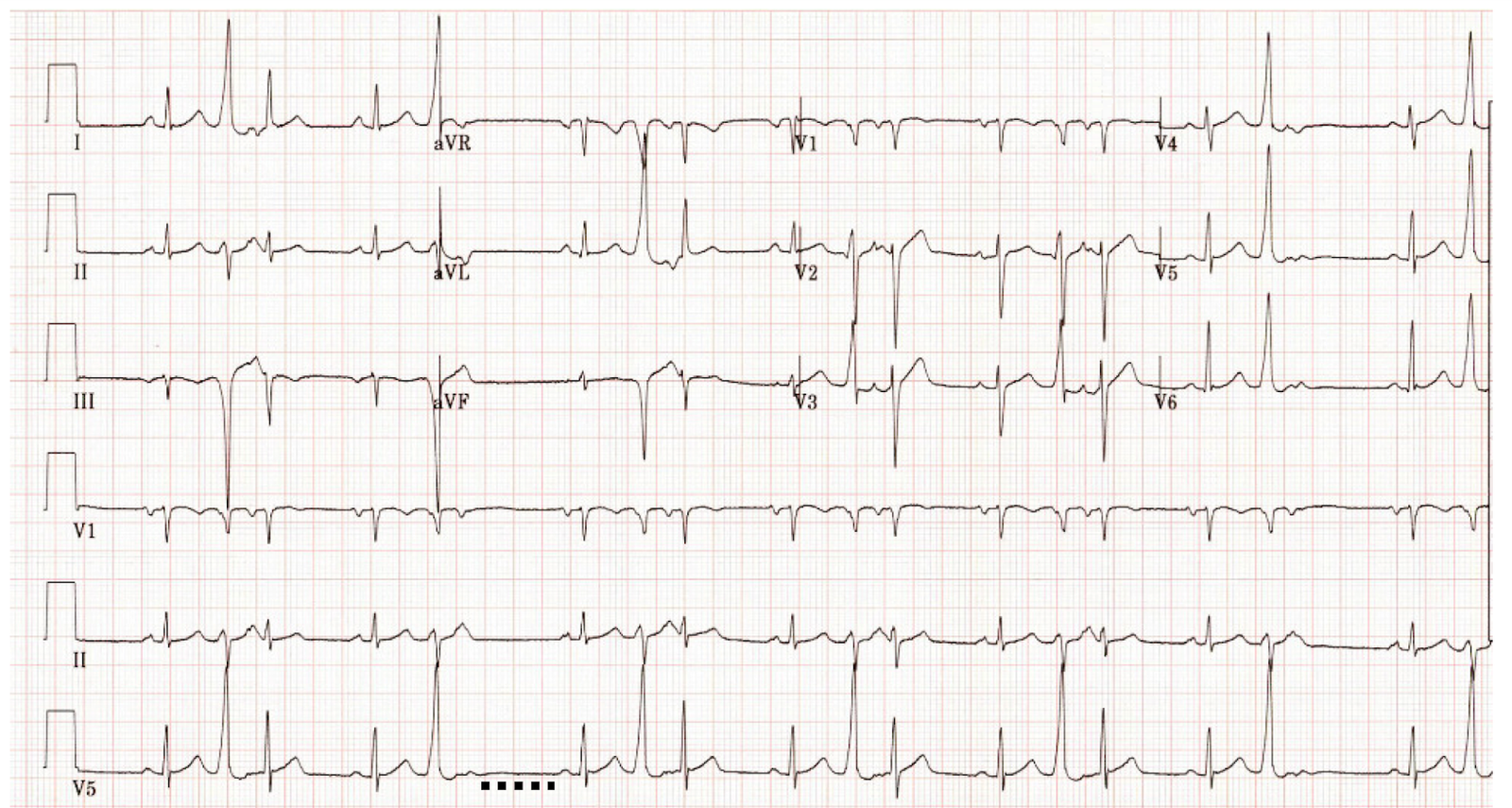
Dr. Grauer has created images for us to understand the morphology of the P waves, as well as a ladder diagram showing the actual rhythm:
 |
| Here we add a red curved line showing the expected morphology of the ST segment and T wave of the PVC, if there had not been a superimposed sinus P wave. With this for reference, you can see that the superimposed P wave is in fact upright in this lead, not inverted. |
 |
| Dr. Grauer’s ladder diagram showing the exact rhythm events. |
Thus, the actual rhythm here is sinus rhythm with frequent, interpolated PVCs, a few of which make the AV node refractory at just the right time to block conduction of a sinus P wave.
There is no pathologic AV block.
The atrial and ventricular beats after the PVCs are not echo beats. An echo beat occurs when a ventricularly originating action potential (in this case, the PVC) proceeds retrogradely up the AV node, then causing a retrograde P wave which can “echo” back down and then proceed anterogradely back through the AV node, causing a narrow complex QRS. These P waves at the end of the PVC are not inverted, therefore not retrograde, and they are timed exactly at the moment when the sinus P waves should occur. They are simply sinus.
Meyers note: I initially thought these were echo beats, until Dr. Grauer pointed this out! A cardiologist was consulted for this ECG who gave a formal interpretation of echo beats as well. Luckily for the patient there was no danger from this rhythm, nor from the incorrect interpretation.
Electrolytes were repleted, PVCs were noted to be much less frequent, and mother and baby did well.
Learning Points:
Interpolated PVCs can sometimes cause the AV node to be refractory at the moment when the next sinus P wave would have conducted, causing physiologically normal blocked conduction. This is not pathologic AV block, but rather normal AV node function.
Echo beats occur when a ventricular action potential goes retrogradely up the AV node, then causes an inverted retrograde P wave, then “echoes” back down to the AV node anterogradely, then resulting in a narrow QRS. This case does not show echo beats, but could be mistaken for them.
Ladder diagrams can help understand and teach rhythms.
Anytime you find waves that march out perfectly, it is always more likely that they are from one source than two. Echo beats that happen to be perfectly timed with the sinus P waves is a stretch of logic, instead of realizing that they are simply all sinus P waves firing perfectly on time.
Thanks to Dr. Grauer for helping me understand this rhythm!
====================================
2 Useful LINKS on today’s topics from Ken Grauer, MD (7/15/2021):
- For a “deep dive” on Echo Beats — CLICK HERE —
- For more on interpolated PVCs — CLICK HERE —
===========================