A man in his 40’s with a h/o coronary disease complained of sudden dizziness and chest pain. Medics found him with a high pulse, and rhythm strip and prehospital 12-lead (not shown) had a wide complex at a consistent rate of 135.
On arrival, here is his initial ED ECG, and is identical to the prehospital ECG and at the same rate:
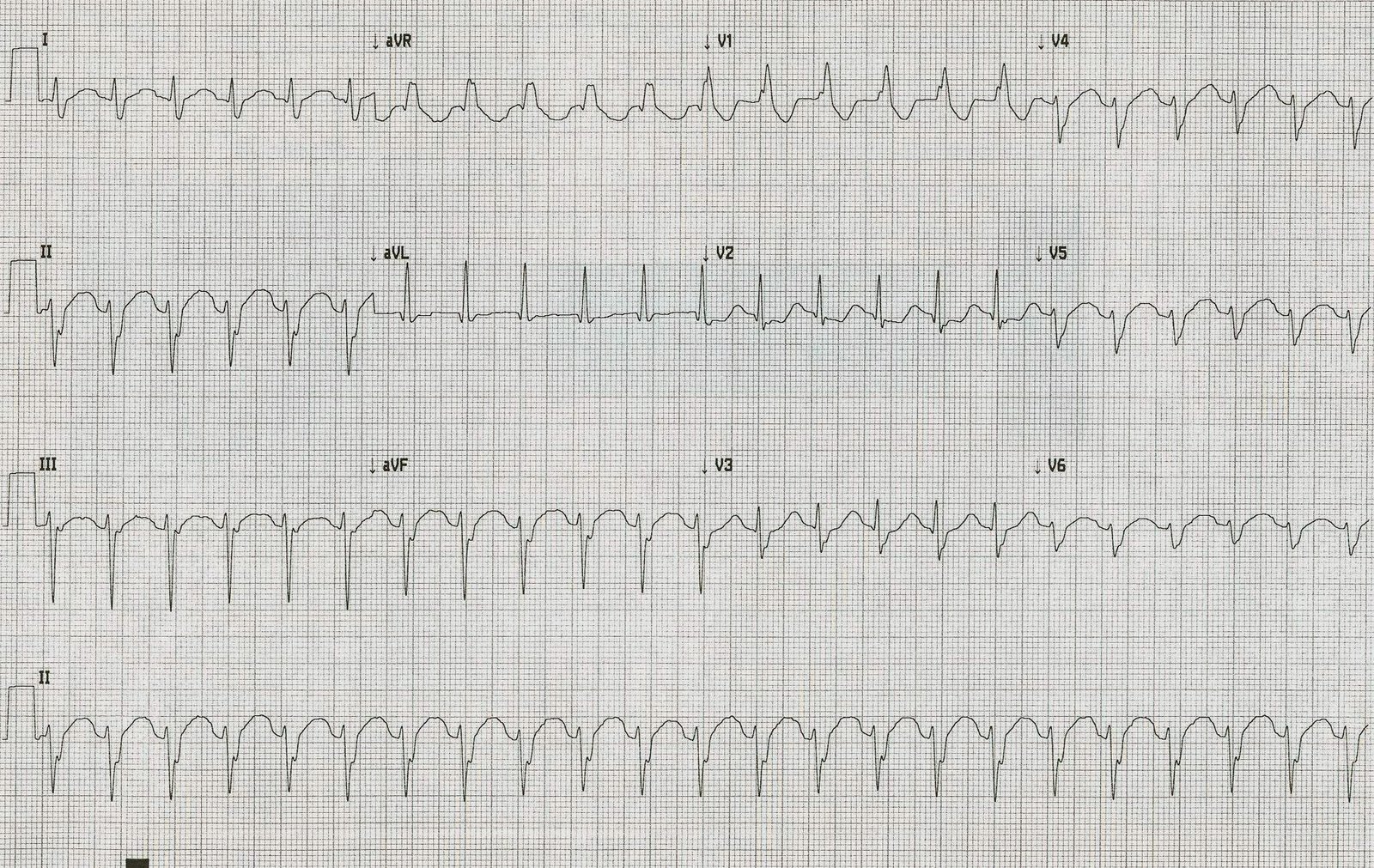 |
| There is a regular, wide complex. No p-waves are seeen. The wide complex has a right bundle branch and left anterior fascicular block morphology. No flutter waves are apparent. |
So this is most likely SVT (PSVT) with aberrancy (RBBB) because: a) the typical RBBB pattern makes VT unlikely b) the absence of p-waves and the constancy of the rhythm makes sinus tach unlikely and c) flutter should have something that could be construed as flutter waves in leads II and/or V1.
Alternatively, it could be posterior fascicular ventricular tachycardia.
Therefore, adenosine was given: the patient responded with several seconds of asystole. No underlying flutter waves were uncovered and no p-waves either. The rhythm gradually returned to its baseline at a rate of 135. So it is not VT, but it was still puzzling. Either the PSVT was broken and restarted, or there is sinus tachycardia.
Just as it describes, I then:
- Placed the Right Arm electrode on the patient’s manubrium.
- Placed the Left Arm electrode on the 5th intercostal space, right sternal border.
- Placed the Left Leg electrode on the right lower costal margin.
- Monitored Lead I.
This is the rhythm strip that resulted:
 |
| Now p-waves are obvious (and large!) |
By changing the lead orientation, one can detect atrial activity with much higher sensitivity. Our electrophysiologist learned of this age-old technique (first described by Sir Thomas Lewis in 1931) technique from his mentor, and also uses it in wide complex tachycardia to detect atrioventricular dissociation (when you see AV dissociation in wide complex tachycardia, it is diagnostic of ventricular tachycardia).
Some Final Comments:
I have added this because of some comments/questions of whether I might treat with verapamil because this looks like verapamil sensitive idiopathic VT:
While this does look like verapamil sensitive idiopathic VT, it does have a typical bifascicular block pattern. The only thing atypical about it is the T-waves in V2 and V3, but the QRS pattern is typical for RBBB + LAFB.
The patient‘s baseline ECG looks exactly the same, except that it is slower (93) and the p-waves are obvious. The Lewis leads proved that it was indeed sinus tach. And with time and fluids and anxiolytics, the rate did trend down.
Sinus tach is usually compensatory to some underlying illness. Maybe the patient has dehydration, sepsis, hemorrhage, or PE. If you were to give verapamil to someone with sinus tach secondary to underlying pathology, you would harm them and perhaps provoke hypotension and shock.
Thus, I would be very careful about giving verapamil to someone with such an ECG until you have proven that it is not sinus tach.
In fact, this is what we did. My resident wanted to treat the presumed SVT with verapamil because it had apparently recurred after adenosine. I expressed my concerns as above, and that is when we did the Lewis leads.
Outcome:
The etiology of the patient’s sinus tachycardia was not discovered. He later returned to the hospital for recurrent bouts of idiopathic sinus tach.
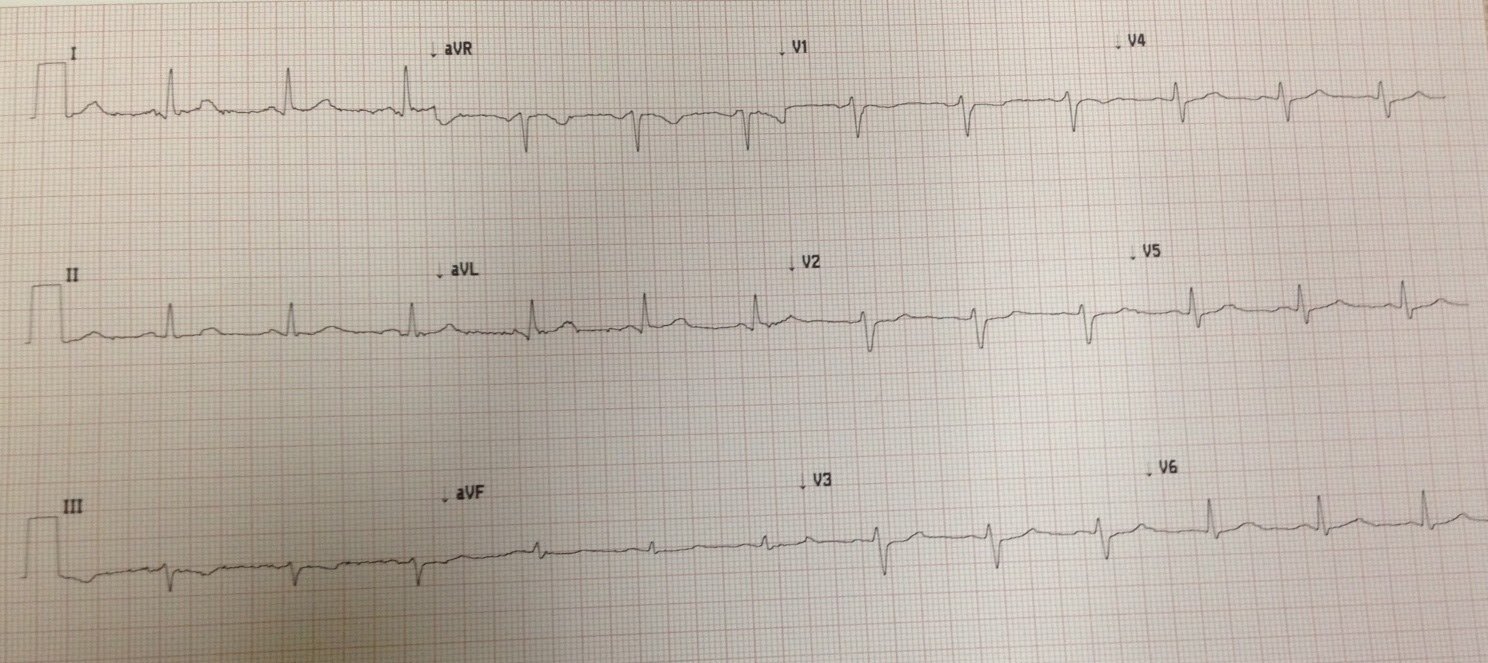
Here is his ECG 24 hours later, at a rate of 118:
 |
| P-waves at this slower rate are now clearly visible. The QRS morphology is identical, confirming that this rhythm had to be supraventricular. The supraventricular rhythm was sinus |
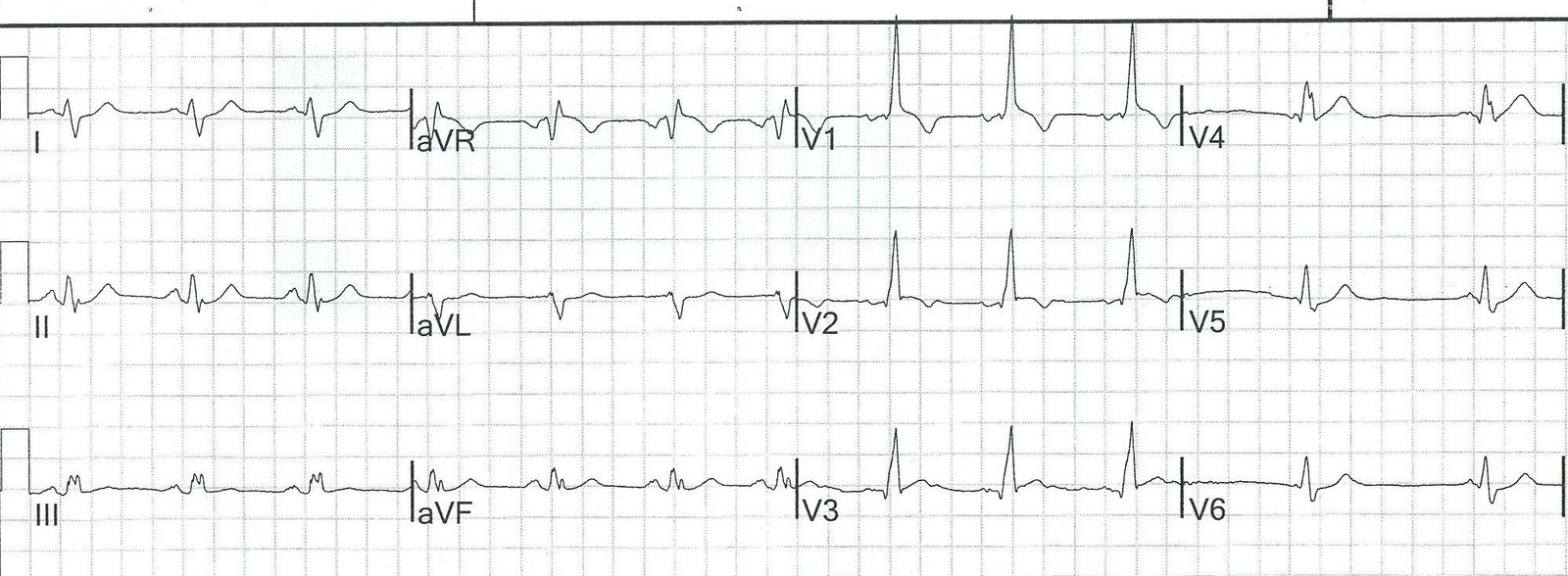
Here is an ECG from 2 weeks later:
 |
| Again, this is clearly sinus rhythm with RBBB and LAFB. |
Learning Point:
When SVT with aberrancy or VT are suspected, both may be ruled out by diagnosis of sinus tachycardia using Lewis Leads. These are simple and fast.