A young woman presented by EMS for weakness.
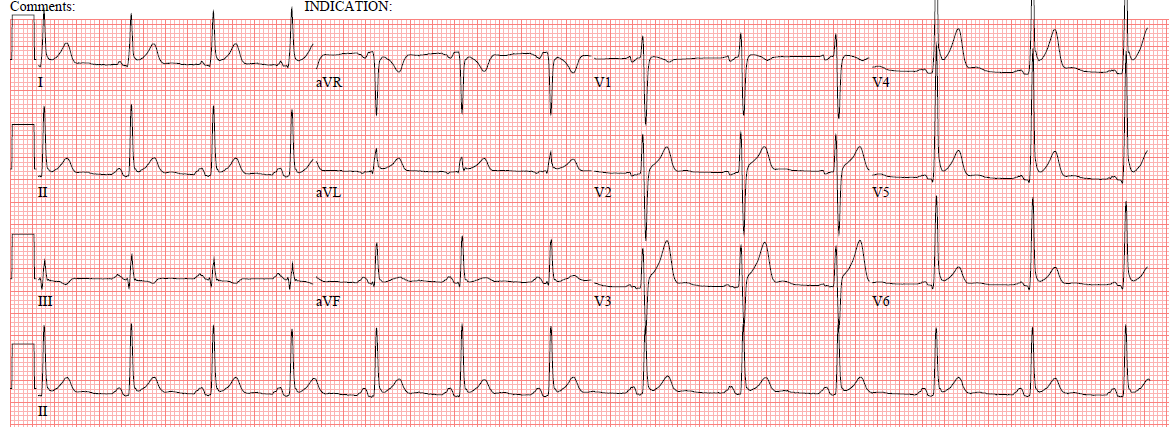
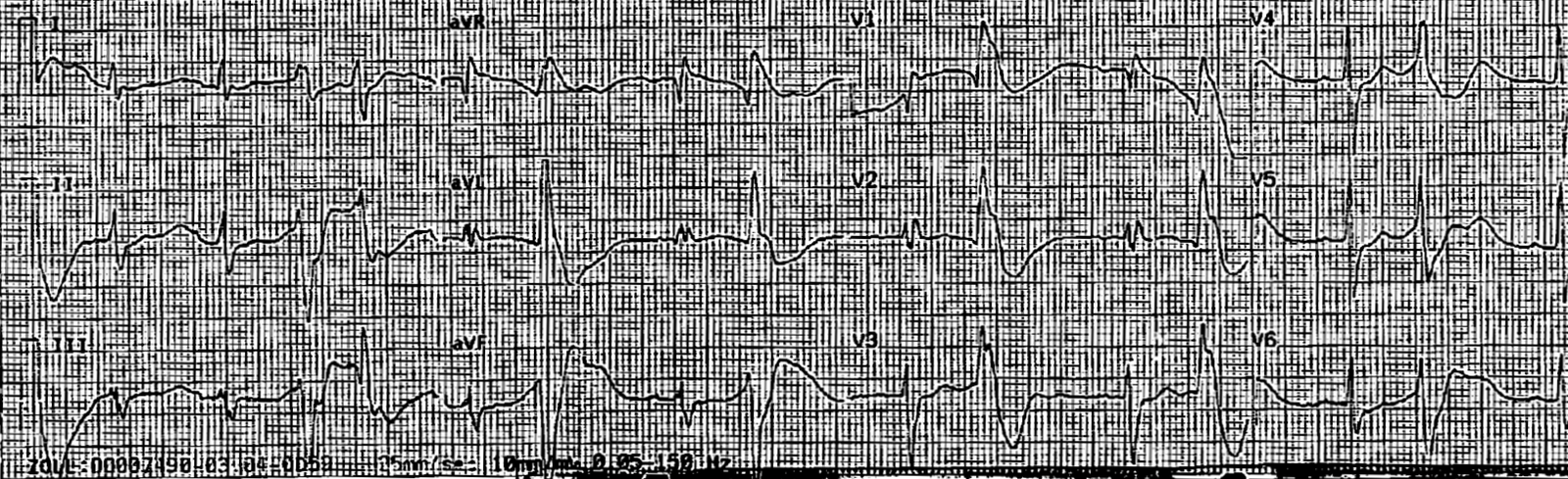
Here is her ED ECG:
 |
| Diagnosis? See Below. |
 |
| There is sinus rhythm. There is a very wide and bizarre PVC. The arrows point to what appear to be very late T-waves. The two black lines show how, if these are T-waves, the QT interval is 600ms and the QTc is then 680ms. This is too long. When the QT is this long, you are seeing U-waves, not T-waves. The blue arrows point to U-waves and the Blue lines show them in simultaneous leads. |
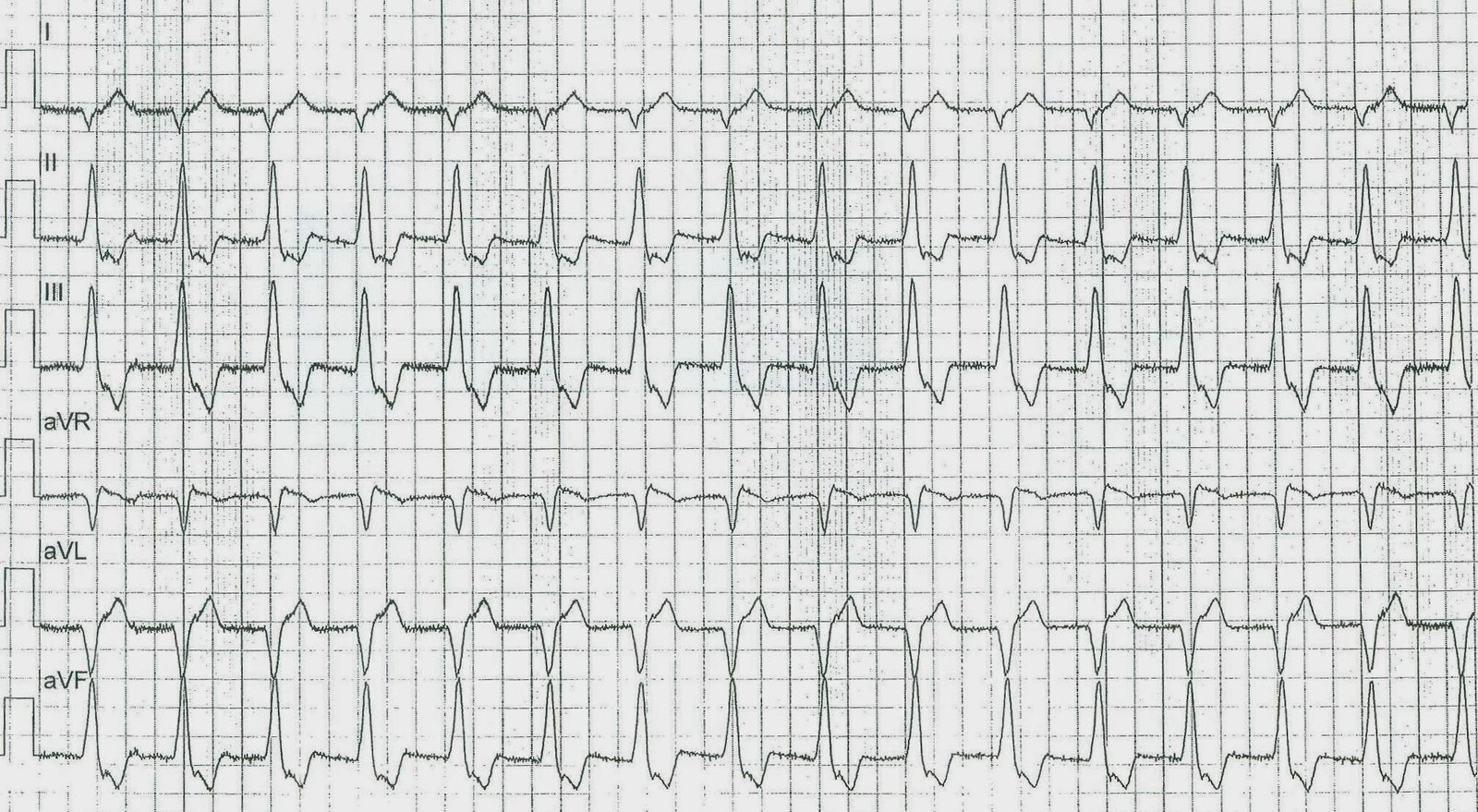
Here is the prehospital ECG:
 |
| This is harder to interpret, except that there are multiple bizarre PVCs demonstrating the cardiac irritability. |
U-waves like this are almost always a result of hypokalemia. They may also be due to drugs that block potassium channels, which simulates hypokalemia.
The patient’s weakness is due to a K of 1.5 mEq/L. This is very dangerous and can lead to ventricular fibrillation, as in this case. It is a true Medical Emergency.
Here are more ECGs of hypokalemia.
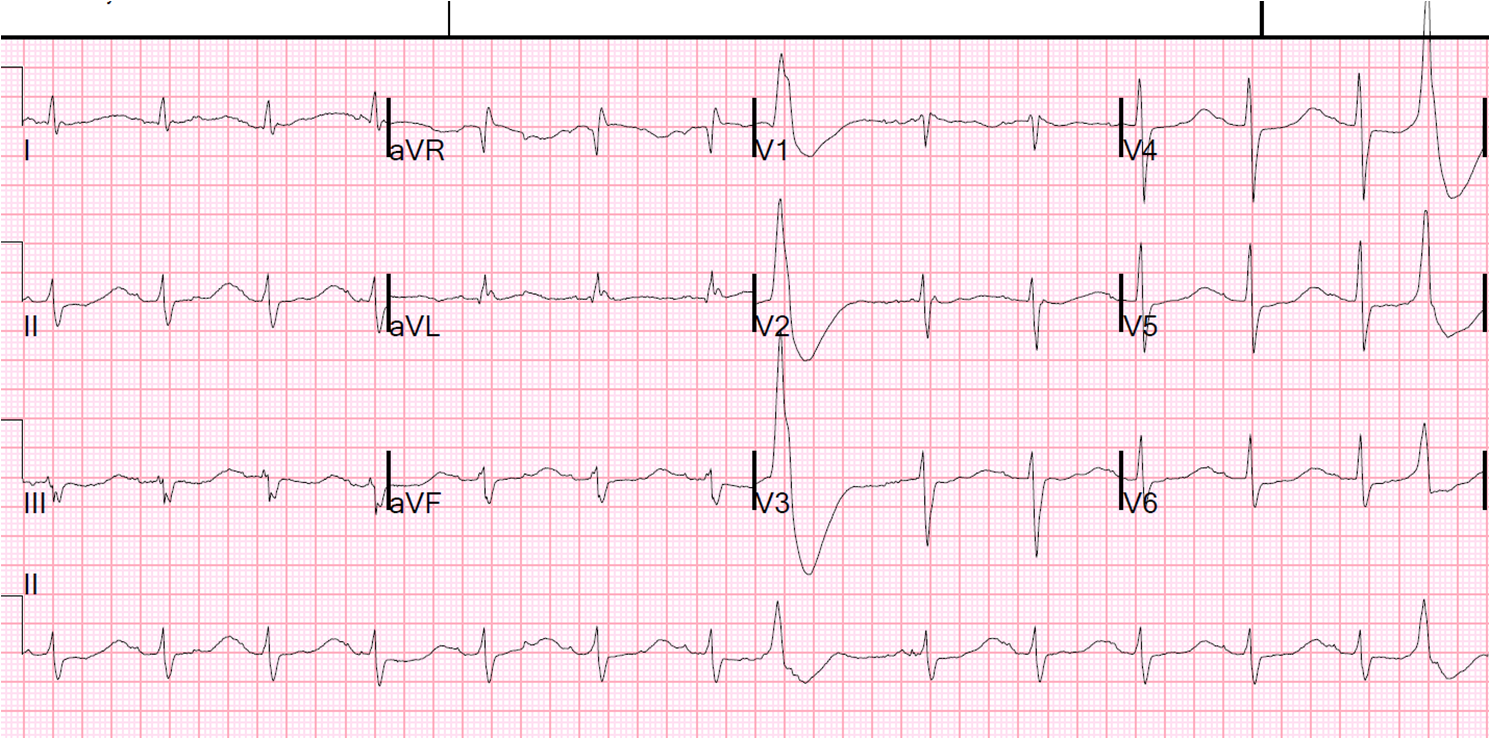
The patient’s K was replenished, and this was the ECG 4 hours later with a K of 4.5 mEq/L: