These 2 ECGs were texted to me with the words “I think acute MI, but cardiology does not.”
I believed these to be 2 serial ECGs:
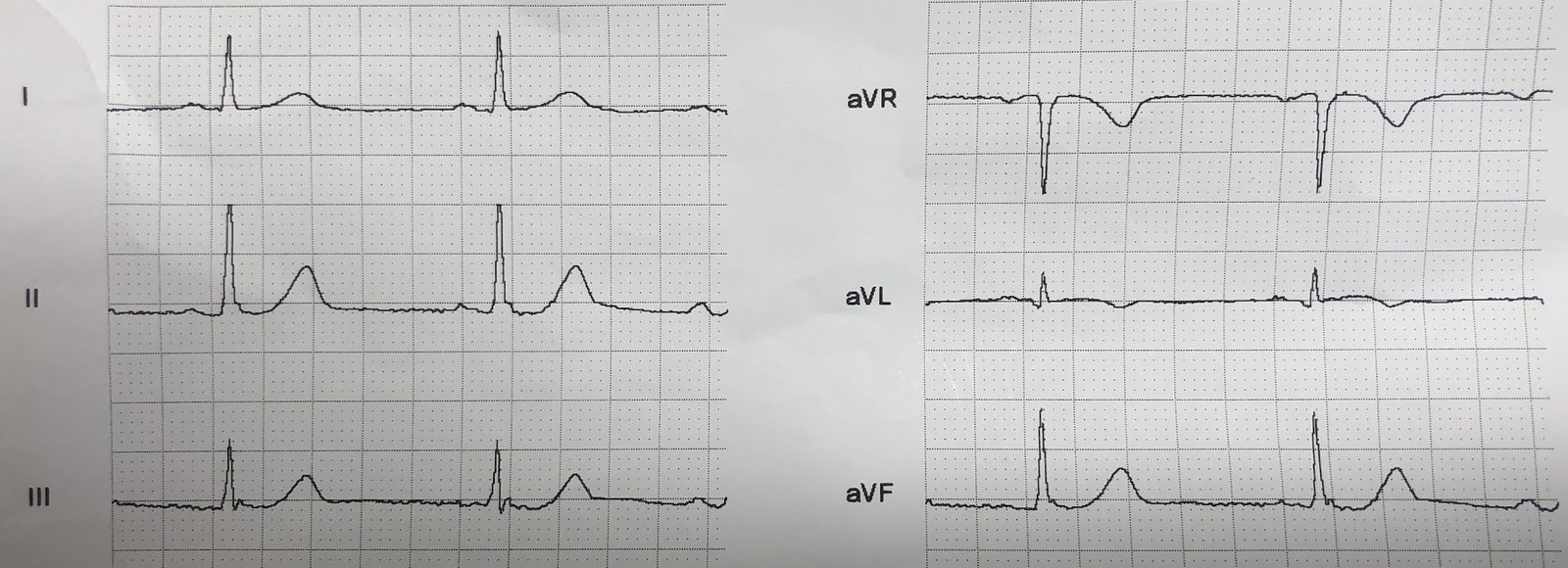
ECG 1: (later found to be time zero):
 |
| Computer read: “minimal ST depression 0.025 mm” There is a small amount of STE in II, III, aVF From less than 0.5 mm – 0.5 mm. There is les than 0.5 mm of reciprocal ST depression in aVL, and an inverted T-wave |
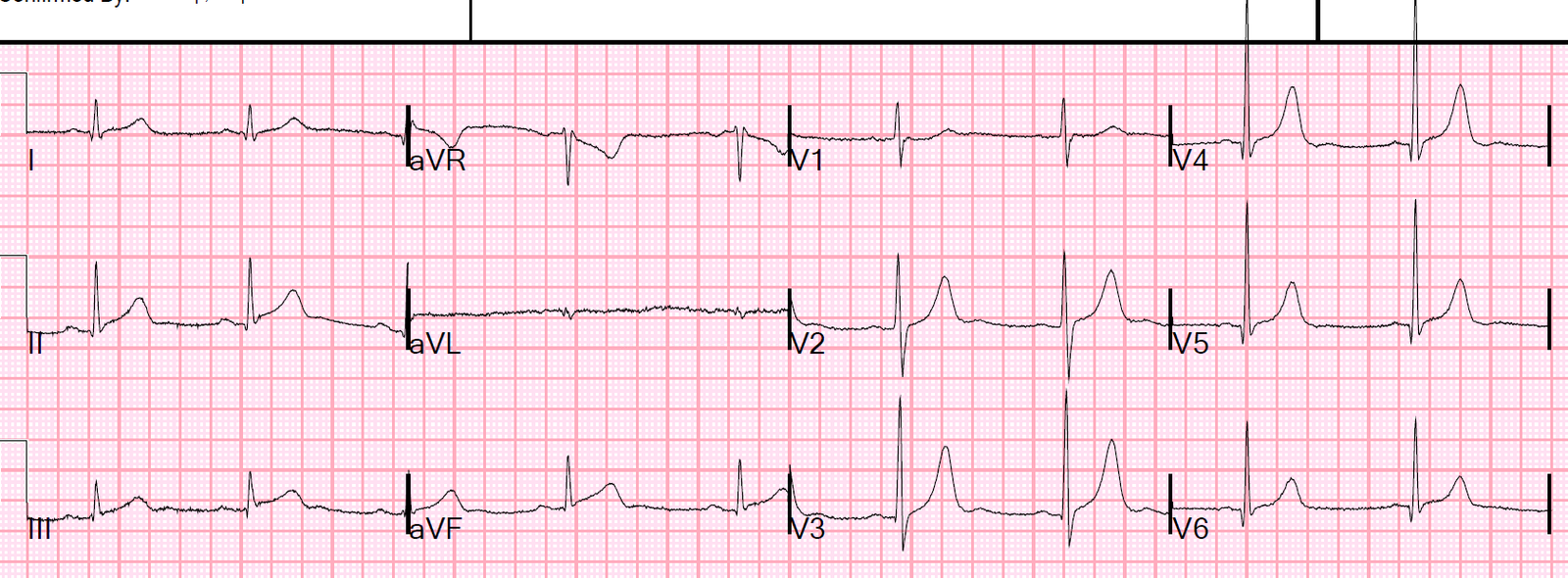
And the other: (later found to be time 24 minutes):
 |
| Now there is more STE and more STD One very telling finding are the ST segments in V2-V6: ST depression has developed in V2-V6, downsloping in V4-V6. Though minimal, this is very specific adjunctive data for ECG diagnosis of MI. |
This was my response:
“It looks like a myocardial infarction…Does the patient have chest pain?”
History:
Syncope in clinic, some vague chest pain.
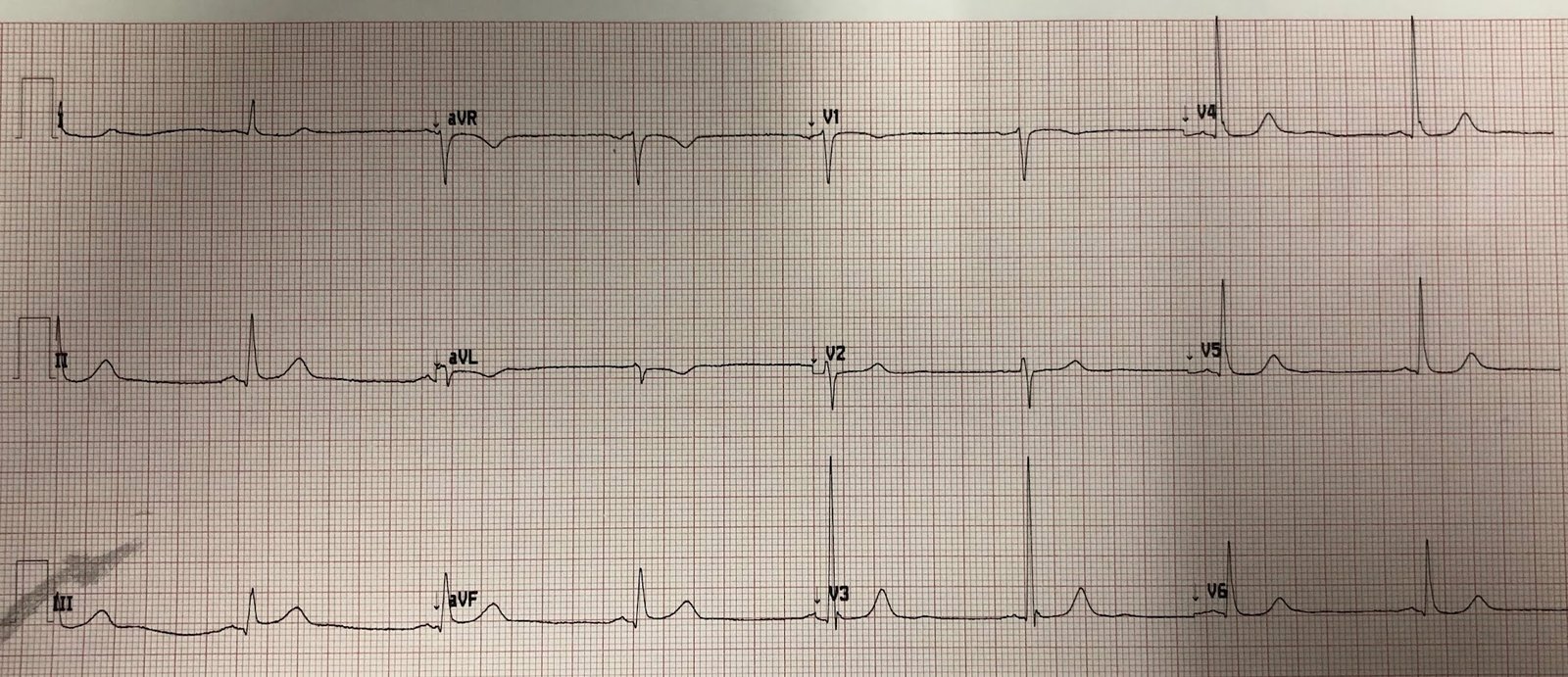
Not a great history, so we looked for a previous ECG:
 |
| From within the last year
No STE, no STD. |
Cardiology had wanted the patient to be admitted, but had not seen evidence of acute MI and had not wanted the cath lab activated.
In spite of this, my partner and I agreed the cath lab should be activated, so he did activate.
Just before transport, another ECG was recorded at time 71 min, prior to cath:
 |
| Now obvious inferior and posterior STEMI. |
The patient had a ventricular fibrillation arrest before the angiogram, and was resuscitated.
Angiogram: 100% distal RCA occlusion.
After cath, next day:
 |
| Reperfusion T-wave in III. STE resolved. |
Peak trop 47.4 ng/mL (large MI)
Echo: Regional wall motion abnormality-inferior, EF 60%.
Learning Points:
1. In the original thrombolytic trials (the only placebo-controlled reperfusion trials!), especially GISSI-1, treatment of inferior MI with streptokinase did not have a measurable effect on mortality outcome. Here we see what appears to be an electrocardiographically tiny inferior MI, which only later becomes large. The patient arrests and has a very high troponin. So don’t be fooled by an apparently small inferior MI.
2. Do serial ECGs.
3. Compare with a previous ECG.
4. You must push to get patients who need it to the cath lab.
5. Cardiologists have a huge amount they have to know, spanning an enormous specialty. They do not always have time to learn the subtleties of OMI on the ECG.
6. You have to be the expert!!
![]()
===================================
Comment by KEN GRAUER, MD (6/23/2019):
===================================
The definition of the word “subtle” is — so delicate or precise as to be difficult to analyze or describe (especially when referring to a change). Subtlety is the “theme” of this case.
- For clarity — I’ve put the first 3 ECGs shown in this case together in Figure-1. Because of how subtle the findings are — I’ve enlarged one complex in leads II, III, aVF and aVL, that I’ve placed to the right of each of these tracings.
 |
| Figure-1: The first 3 ECGs shown in this case — with enlargement of leads II, III, aVF and aVL to the right of each tracing (See text).
The CASE: ECGs #1 and #2 in Figure-1 were texted to Dr. Smith with the words, “I think acute MI — but cardiology does not… “
My THOUGHTS on ECG #1 — The rhythm appears to be regular, at a rate just under 50/minute. The QRS is narrow. This is sinus bradycardia.
Regarding Q–R–S–T Changes:
My IMPRESSION: I was not at all certain about what was going on after looking at this initial ECG ( = ECG #1). My concerns were the following:
Looking at the BLOW-UPS (magnified views) of Leads II, III, aVF and aVL for ECG #1 and ECG #2:
|