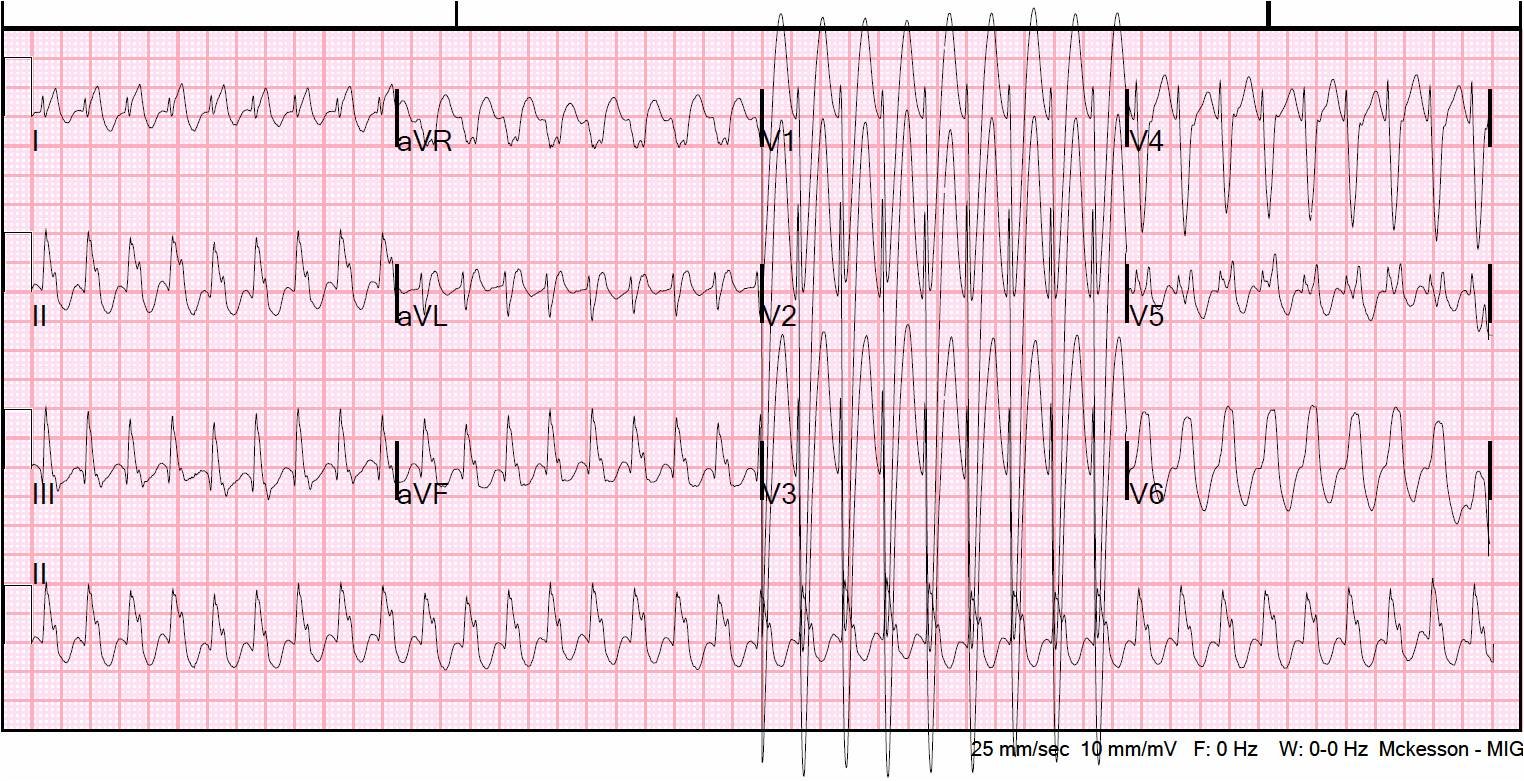
This 49 yo black male presented with sudden substernal non radiating pleuritic chest pain on the day prior to presentation. Here is the presenting ECG:
 |
| There is ST elevation in anterior leads that is classic for early repolarization: there is excellent R-wave progression, QT is not long, T-waves are assymmetric (slower upstroke than downstroke), and well-formed J-waves. The equation value [1.196 x (ST elevation at 60 ms after the J-point)] + [QTc x 0.059] – [R amplitude in V4) x 0.326)] is low [= (2.0 x 1.196) + (418 x 0.059) – (25 x 0.326)], which is equal to 18.9. A value less than 23.4 is unlikely to be MI. Interestingly, the presence of J-waves did not add value to the prediction rule equation. |
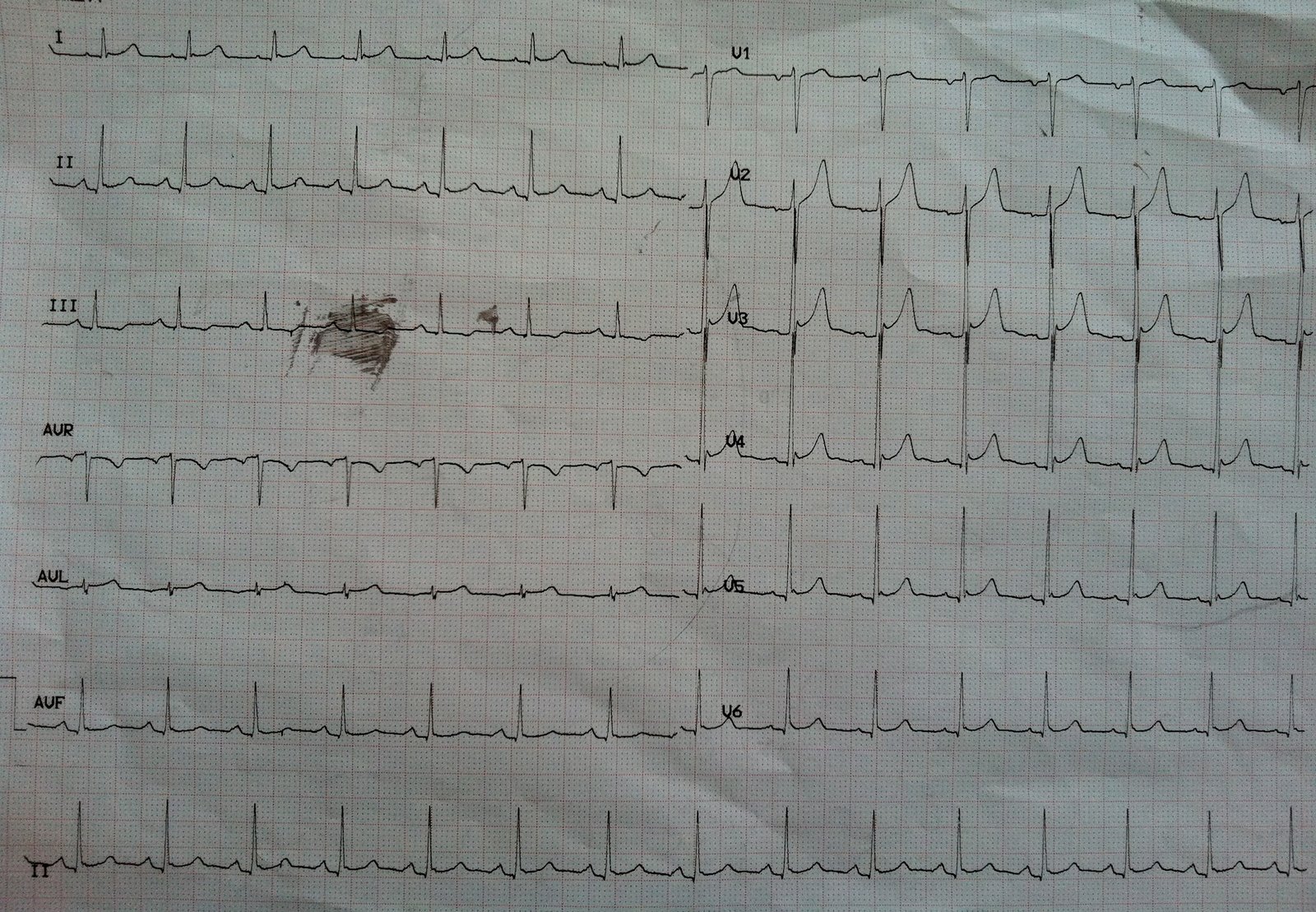
Bedside ultrasound showed no wall motion abnormality. A troponin drawn the next AM was negative. A repeat EKG showed increased ST elevation:
 |
| Equation value is: (4.5 x 1.196) + (0.059 x 400) – (0.326 x 28) = 19.9 (early repol) |
Repeat echo again showed no wall motion abnormality.
Why is the ST elevation greater in the second ECG? One must remember that the ST elevation of early repolarization diminishes with increased sympathetic tone, such as during exercise. When the heart rate is faster, as in the first ECG, the ST elevation is likely to be less pronounced than when the heart rate is slower.
Kambara found in his longitudinal study of patients with early repolarization that, in 26% the ST elevation disappeared on follow up ECG and in 74% the degree of ST elevation varied on followup ECGs.
I do not have proof in this case, but I’m pretty certain that the difference in ST elevation is due to the difference in heart rate.
Learning point: The ST elevation of early repol is not constant. In particular, it may be diminished with exercise, sympathetic tone, and heart rate, and may be increased when the heart rate is slower.
Thanks to Steve Dunlop for this case.
Here is a good review article on early repolarization: