An elderly woman had syncope while having a bowel movement. She had an aortic stenosis murmur. Here is her ECG:
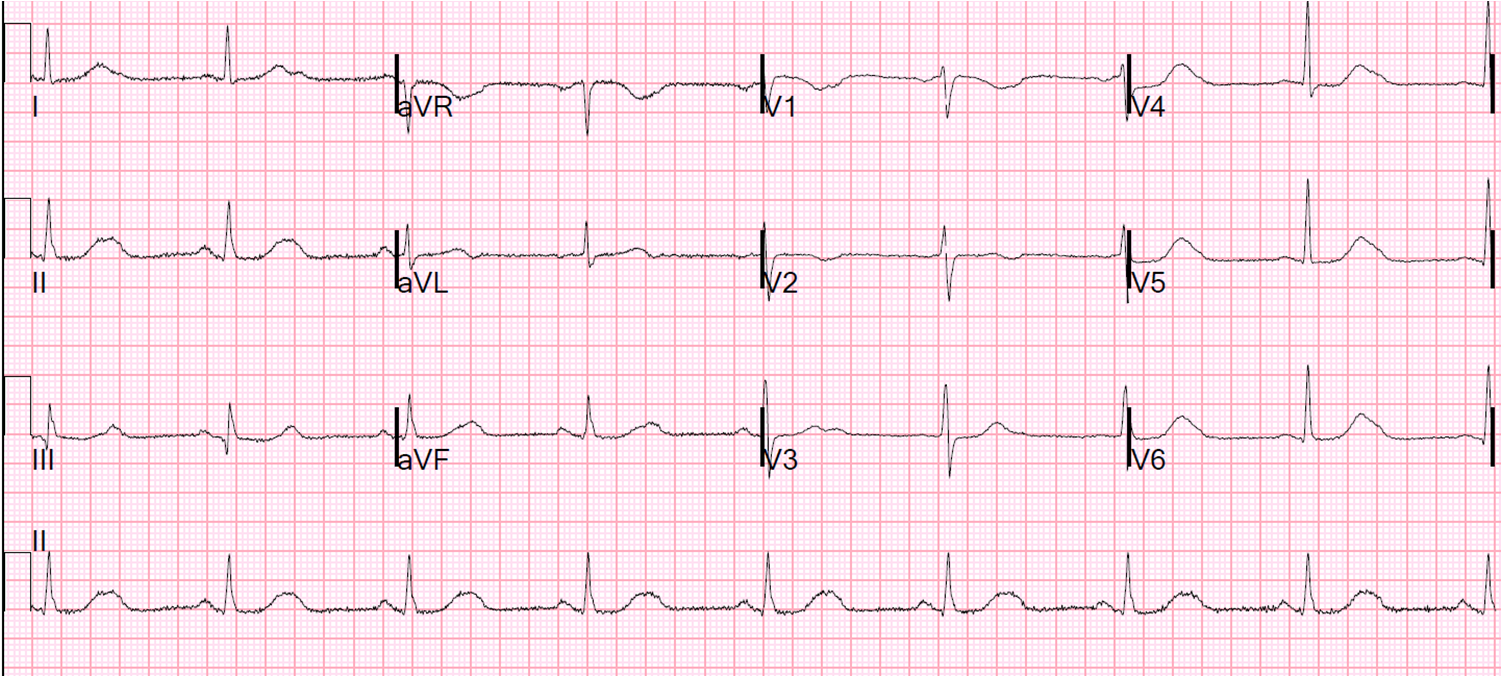 |
| Computer only read sinus bradycardia. Anything else?
Or are there P-waves buried in the T-waves, and this actually 2nd degree AV block, Mobitz II? Computer Measurements: |
The differential of her syncope was listed initially as:
–sick sinus syndrome (because of the bradycardia)
–normal sinus, but 2nd degree AV block, Mobitz II
–aortic stenosis
–Valsalva syncope (on the toilet)
What is the most important entity missing from this differential?
Long QT. Again, the computer fails at measuring the QT interval. Here is another case I recently posted.
Here is a manual measurement in lead V5. One measures this be drawing a line along the downward slope of the T-wave until it intersects with the baseline:
 |
| From the beginning of the QRS (vertical line) to the end of the T-wave (slanted line) is 15.75 little boxes, each of which is 40 ms. 40 ms x 15.75 = 630 ms |
The preceding R-R interval is 1200 ms = 1.2 sec. The square root of 1.2 is 1.095. The QTc is then: 630 divided by 1.095 = 575 ms
The computer read a QTc of 442 ms (vs. our manual measurement of 575 ms!!)
Sometimes, what appears to be a prolonged QT is really a QU interval (a U-wave is making it appear as if there is a long QT). Is that the case here? No.
Case Progression:
The patient was given 2 g of IV Magnesium. A Mg level returned low at 1.2 mEq/L. The patient was admitted to telemetry. More Mg was given until the level was up to 2.2 mEq/L.
While on telemetry, she had a 12 second episode of Torsade de Pointe. She also had several runs of Non-sustained VT and many PVCs. Echo showed only moderate aortic stenosis.
She was found to be on a couple antibiotics that can prolong the QT interval. More magnesium was given. There was a plan for isoproterenol infusion should this recur.
See here for full management of Polymorphic Ventricular Tachycardia.
Again, the computer measurement of QT interval fails. The computer does well at measuring QT intervals of less than 450 ms. I have been unable to find studies of the accuracy of computerized QT interval when it is long. But in my very long experience, and paying a lot of attention: when the QT is long, the computer usually fails to register this abnormality.
Lesson:
1. You must assess the QT interval visually. If it appears long, then measure it manually (in the lead in which it is longest). A QTc interval greater than 500 ms is potentially dangerous.
2. Acquired long QT is more likely to cause torsade when the patient is bradycardic (“pause dependent”). A longer pause creates a longer QT interval, allowing more time for a PVC to land on the vulnerable part of the T-wave. Thus, increasing the heart rate with isoproterenol or overdrive pacing prevents Torsade.
3. Although a slow heart rate results in a shorter QTc (corrected for heart rate), it also leads to a higher risk of Torsade at any given QTc!