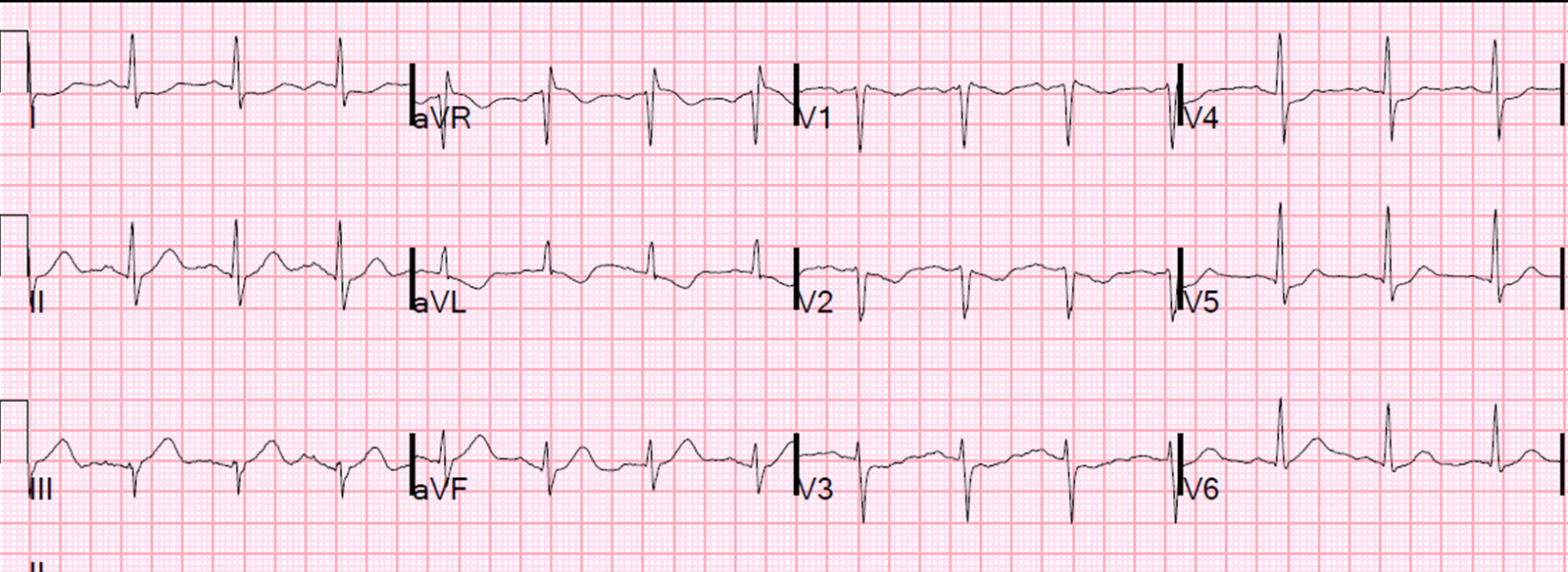
A 70 year old diabetic complained of 6/10 epigastric pain. Here is his initial ECG:
 |
| There is diffuse ST elevation: II, III, aVF and V3-V6. There is reciprocal ST depression in aVL. This is diagnostic of inferolateral STEMI |
The emergency physician activated the cath lab and gave appropriate antiplatelet and antithrombotic therapy.
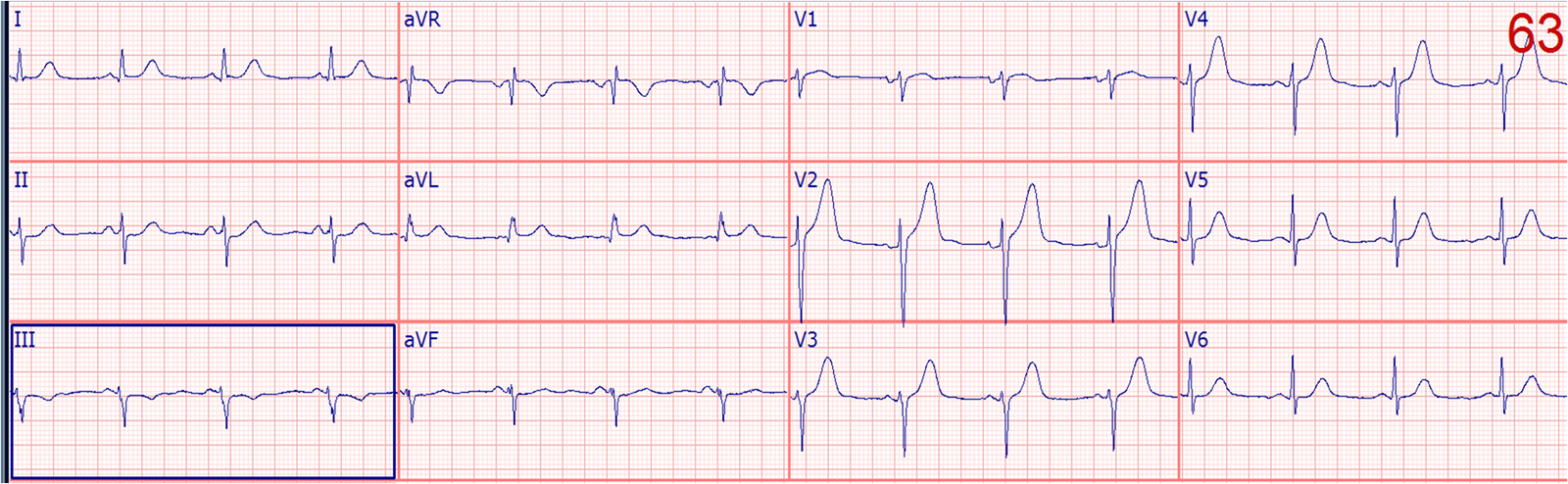
The PCI team came to talk to the patient, and while they were talking, the patient vomited and was pain free thereafter and said he felt much better. They recorded another ECG:
 |
| The ST elevation is resolved. There can be no other explanation than the patient spontaneously reperfused an occluded coronary artery. |
The cath team cancelled the angiogram. They admitted the patient to a floor bed. I do not have any insight into what they were thinking. Did they think it was pericarditis? If so, pericarditis does not suddenly resolve. Did just ignore the first one? Or did they think that since the ST elevation resolved that this did not need emergent cath?
As it turned out, the patient ruled out for MI by serial contemporary troponins. They were about to discharge him to home when an emergency physician objected. He called the inpatient team and expressed his concerns, and to at least do a CT coronary angiogram or a stress test before discharge.
They consulted the cardiologists again and this time they took the patient for an angiogram.
Angiogram: 80% thrombotic occlusion of the circumflex, stented.
Imagine what might have happened if the fleeting ST elevation had not been recorded on that one ECG? There are those who say that Unstable Angina no longer exists and that we should not be doing further testing on patients who rule out for MI.
Eugene Braunwald argues for a Requieum for Unstable Angina.
Here are many other unstable angina cases.
Transient STEMI, or, as in this case, Transient ST elevation Unstable Angina.
I have seen many cases of transient STEMI with negative biomarkers. Technically, these are not MI by the Universal Definition of MI, which requires at least one elevated troponin, with appropriate rise and/or fall. They are thus really unstable angina with ST elevation. In any case, they are very high risk lesions.
See this case where I screwed up and the patient died.
I am aware of 2 studies on Transient STEMI:
Ownbey M. et al. Prevalence and interventional outcomes of patients with resolution of ST-segment elevation between prehospital and in-hospital ECG. Prehosp Emerg Care 18(2);174-9. Apr-Jun 2014.
They found 293 total cases of prehospital STEMI, but could only find all the relevant records in 83 cases (28%). ST Resolution (STR) by the time of ED arrival occurred in 18 of 83 cases. There were no differences between STR and non-STR cases in prehospital vital signs or treatments. 95% of patients underwent cardiac catheterization with a mean door-to-needle time of 57 minutes (interquartile range 43-71). Comparing STR and non-STR cases, significant lesions (greater than or equal to 50%) were found in 94 and 97% of patients (p = 0.6), and subtotal or total lesions (greater than or equal to 95%) were found in 63% and 85% (p = 0.1), respectively.
Meisel SR, et al. Transient ST-elevation myocardial infarction: clinical course with intense medical therapy and early invasive approach, and comparison with persistent ST-elevation myocardial infarction. Am Heart J 155(5):848.
They studied 1244 consecutive STEMI patients. 63 (5%) had Transient STEMI (TSTEMI): Patients with Transient STEMI were treated with intravenous isosorbide dinitrate, aspirin, and clopidogrel, and/or with glycoprotein IIb/IIIa inhibitors. Coronary angiography performed 1.5 days after admission demonstrated no obstructive lesion or single-vessel obstructive disease in 43 patients (70%). PCI was performed in 48 patients (77%), and 8 patients (13%) were referred to surgery. Left ventricular ejection fraction was within normal limits, and peak creatine kinase was mildly elevated. Transient STEMI was associated with less myocardial damage, less extensive coronary artery disease, higher thrombolysis in myocardial infarction flow grade in culprit artery, and better cardiac function. These data suggest that immediate intense medical therapy with an early invasive approach is an appropriate therapy in patients with Transient STEMI.
The key is that all patients were treated with antiplatelet and antithrombotic therapy, and they generally underwent angiography.
Management of Transient STEMI: My opinion from experience and the literature:
1. Patients with transient ST elevation should go to the cath lab emergently just as if they had not had resolution of ST elevation.
2. If for some reason the angiogram is delayed, they should get maximal medical therapy, be admitted to an ICU, and continuous 12-lead ST segment monitoring. This is because re-occlusion is not always accompanied by symptoms. See this case of asymptomatic re-occlusion.