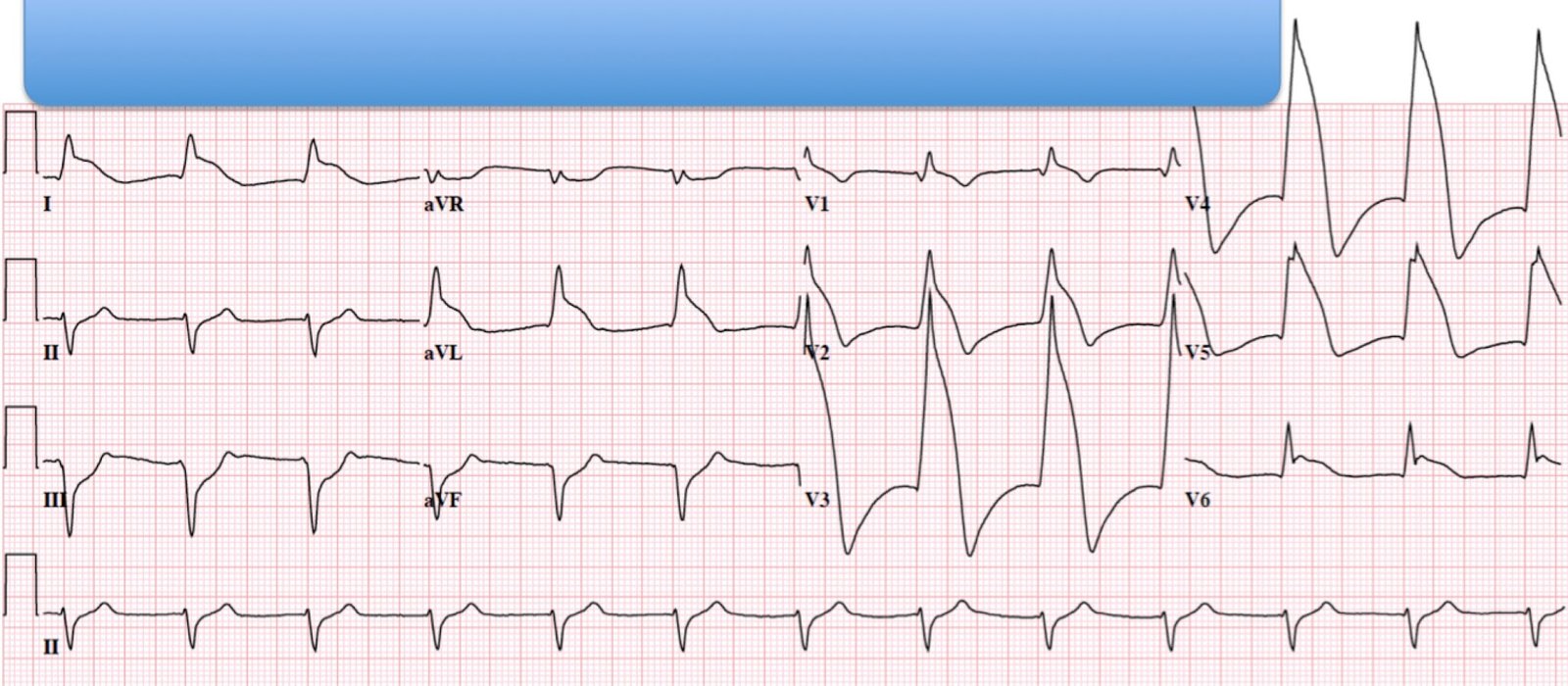
A male in his 40s presented with decreasing chest pain. Here was his first ECG:
 |
| There is sinus rhythm. The QTc is 379 ms. There is ST elevation in V2-V4 that does not meet STEMI “criteria” of at least 1 mm in 2 or more leads (except V2 and V3, which require 2.0 mm of more for men over age 40). So it looks like early repolarization. |
The clinicians used the subtleSTEMI formula (sidebar excel applet). I am not sure exactly what numbers they used, but they told me the value they arrived at was 21.2.
Let’s examine that:
The computerized QTc was 379 ms.
The R-wave amplitude in lead V4 is from 11-14 mm, depending on the complex used.
Here is a magnification of V3 in order to measure ST elevation at 60 ms after the J-point in lead V3:
 |
| The black arrow shows the J-point. The red arrow is at 60 ms (1.5 small boxes) after the J-point. The lower edge of the upper green line is where one should measure from. The upper edge of the lower green line is at the PQ junction. The distance between these two is 4 mm. Some might say 3.5 mm |
If we put these values into the formula, we get 6 different values depending on the measurements:
RAV4 = 11 (min) RAV4 = 12.5 (avg) RAV4 = 14 (max)
_________________________________________________________________________________
STE = 3.5 mm 22.96 22.5 22.0
STE = 4.0 mm 23.56 23.1 22.6
Only one value is very specific for LAD occlusion (23.56, greater than 23.4)
All the rest are greater than 22.0, above which one should definitely be worried and get serial ECGs.
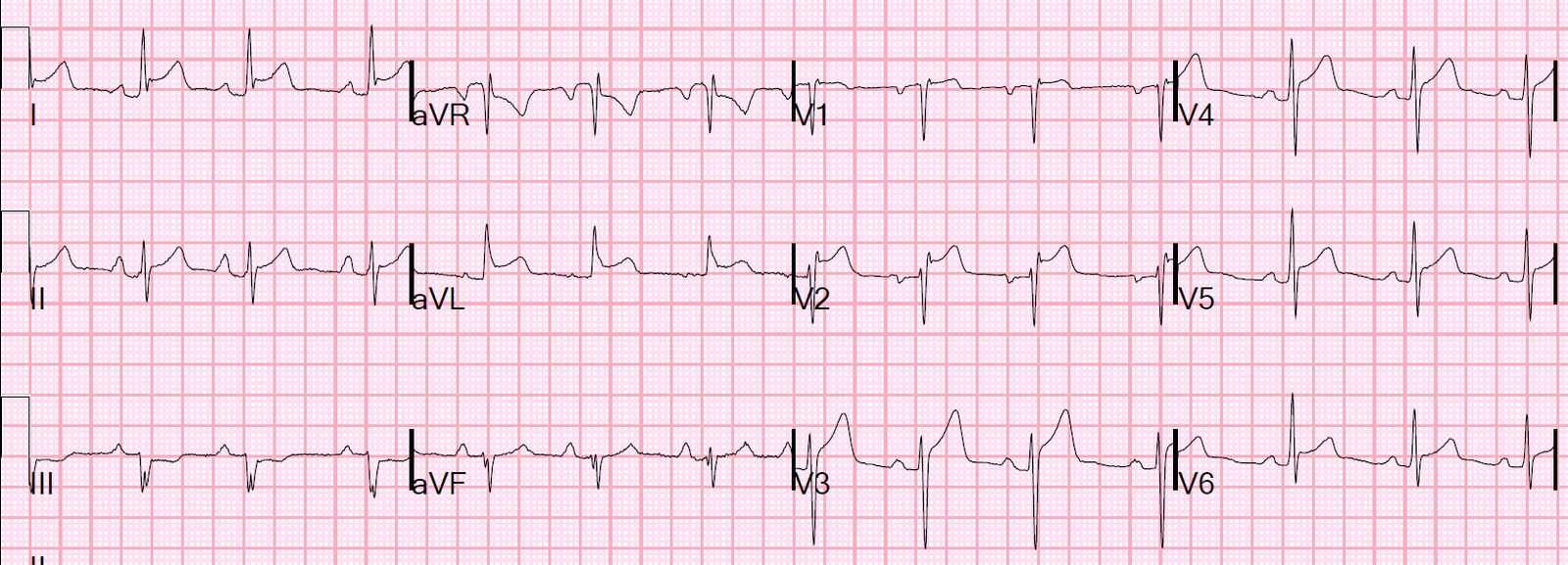
So a second ECG was recorded 12 minutes later:
 |
| QTc is now 383 ms. STE 60 V3 = 3.5 mm. RAV4 = 11-12 mm. |
Formula value is now slightly lower.
These two ECGS are significantly different, but it was not noticed the treating physicians.
Look at the ECGs side by side. And remember the pain is waning.
 |
| The first is on the left, the follow up is on the right. The T-wave amplitude in V3 is 10 mm on the earlier and only 7 mm on the later one. |
This makes it almost certain that the ST elevation on the first one is due to ischemia.
Although the clinicians were uncertain and obtained a very low formula value for both, they were worried about the patients symptoms and appropriately activated the cath lab.
The angiogram showed a 99% thrombotic occlusion with TIMI-II flow (enough coronary flow to prevent outright ST elevation).
It is probable that the artery was fully occluded at the time of maximal chest pain.
Learning Points:
1. Hyperacute T-waves diminish in size as the artery reperfuses
2. The formula is more likely to be falsely negative when there is a reperfusing artery.
3. A value less than 23.4 but still greater than 22.0 may still be due to LAD occlusion or near-occlusion.
4. Serial ECGs are critical but they must be scrutinized for changes, which may be very subtle (see below).
Here is another case in which the T-wave subtly diminishes as the LAD spontaneously opens and pain diminishes (the first 4 are prehospital ECGs):