An anonymous paramedic sent this.
A 60-something with past history only of colon cancer called 911 for non-specific generalized malaise.
The medics state that he was ill appearing.
They recorded an ECG:
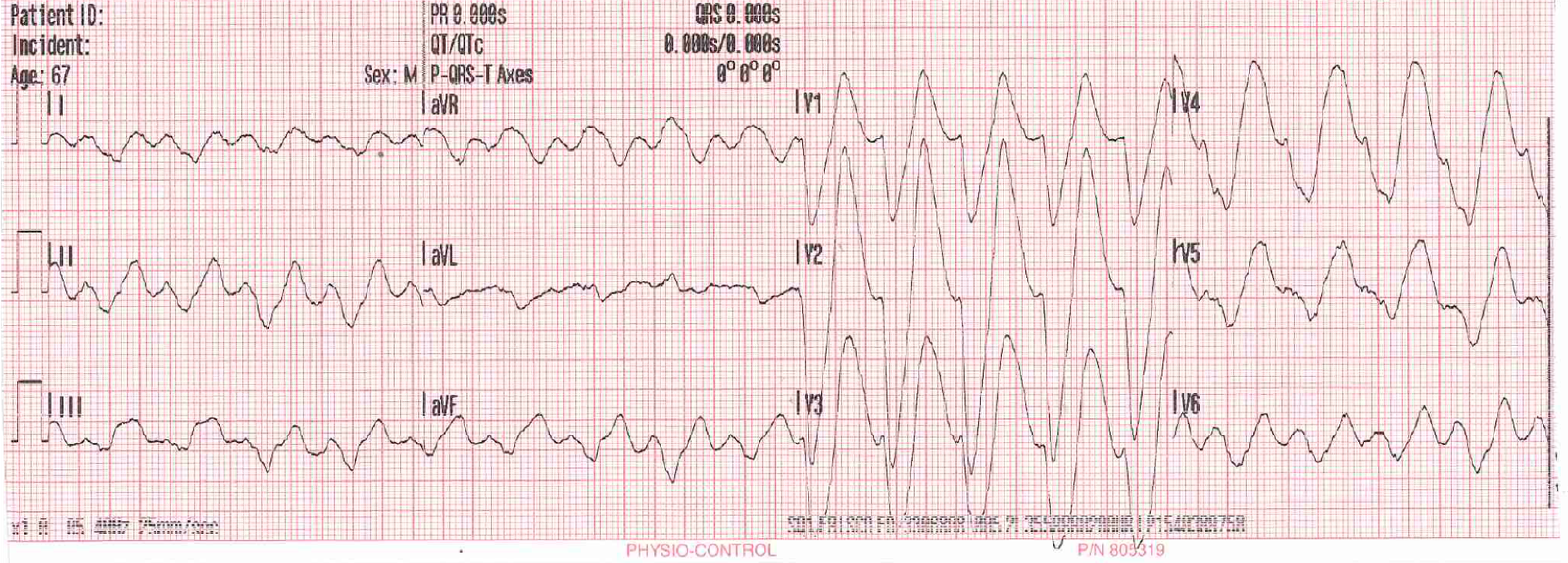 |
| What do you think? |
This is extremely wide, and even if it is VT, it is so wide that there must be hyperkalemia or a severe Na channel blocking overdose. The patient was not on a sodium channel blocker.
The paramedic knew instantly what it was (he credits his regular reading of this blog!)
The patient was only a couple blocks from the hospital, so there was no time for treatment before arrival.
K was 8.9 mEq/L.
Etiology was a combination of NSAID and obstructive nephropathy, with a Cr > 20 (!). Estimated GFR of 2.0.
The potassium was brought down and the patient ultimately did well.