A 50-something male with a history of COPD and substance use disorder who presented with generalized weakness and exacerbation of chronic back pain that is now radiating to his neck, and headache. He also developed nausea, alternating “hot and cold flashes”, and generalized weakness the previous evening. He became anxious about his symptoms and then used crack cocaine as well as drank alcohol last night. His symptoms have persisted since then. He states he has felt short of breath since last night. He denies any chest pain, though notes he has a “odd” sensation in his chest.
Vital signs were normal and physical exam was unremarkable
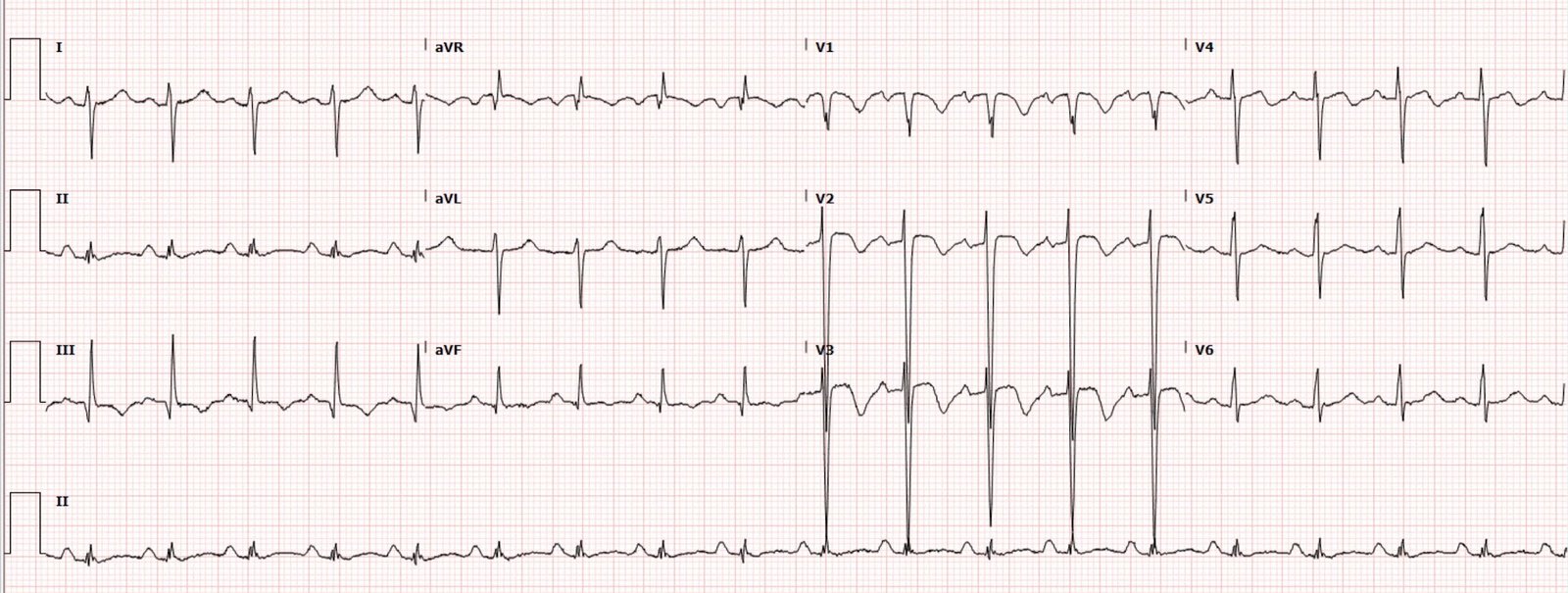
He had an ECG recorded:
This is RBBB, which normally does not have ST Elevation anywhere. In fact, it normally has ST depression in V1-V3 that is discordant to the previous R’-wave.
In this case, there is no R’-wave in V1, which is unusual in RBBB.
V2 and V3 do have rSR’, and both of those also have ST elevation that is concordant to the R’-wave. This usually is an indicator of LAD occlusion.
This is all but diagnostic of lead V1 – lead V3 lead reversal
Nevertheless, the T-waves appear hyperacute.
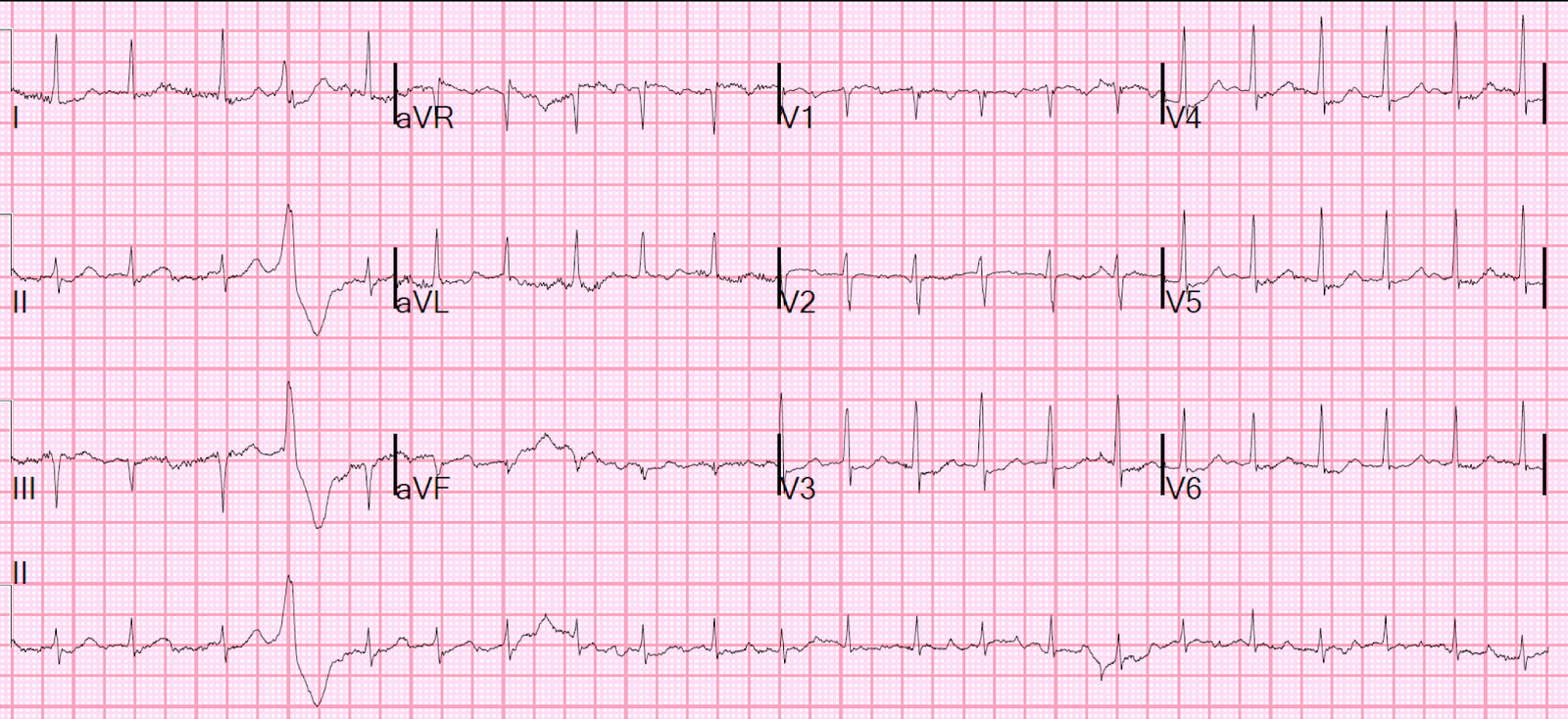
There was a previous ECG from 3 months prior

This ECG does have an R’-wave in V1, and (appropriately) without STE. V2 and V3 are lacking an R’-wave; in fact, they have a wide S wave which is usually only seen in lateral leads of RBBB. There is STE which is discordant to that wide S-wave; usually the ST segment in RBBB is isoelectric even AFTER the wide S-wave.
So this is an abnormal baseline ECG, but the acute ECG looks far more worrisome.
Let’s look at V1-V3 side by side, presentation ECG on the left and old one on the right:

V1 T-wave sure looks hyperacute compared to the old one.
I have not applied the term “Terminal QRS distortion” to RBBB, but if one did so, then the acute ECG would definitely qualify in lead V3 (R’-wave does not return to baseline).
A Bedside echo (POCUS) was recorded:
Notice only the apex contracts; the base does not.
Is it just an apical wall motion abnormality due to LAD occlusion?
One might think so.
Angiogram:
–Large RCA without significant disease.
–Left main is large with mild proximal plaque
–Circumflex is a small caliber vessel and supplies two small OM branches
–There is a medium caliber, multi-branching ramus intermediate without
significant disease.
—LAD is a large caliber vessel that extends to the apex. No significant coronary artery disease is noted in the LAD, but the LAD is noted to dilate with IC nitroglycerin. LAD supplies four small caliber diagonal branches
–Left ventricular end diastolic pressure (LVEDP) 24-27 mm Hg (elevated) in the setting of SBP < 85
Impression and recommendation:
–No significant obstructive coronary artery disease to explain elevated troponin, dyspnea and ECG changes
–No evidence for plaque rupture or vessel occlusion
—Significant elevated left ventricular filling pressure in the setting of relative hypotension
–Consider non-ischemic cardiomyopathy; troponin elevation could be caused by decrease coronary perfusion pressure in the setting of elevated LVEDP. Would not recommend further treatment of ACS
Contemporary troponin I peaked at 0.393 ng/mL, which is typical for a Non-OMI, but also for a variety of “acute myocardial injury” diagnoses.
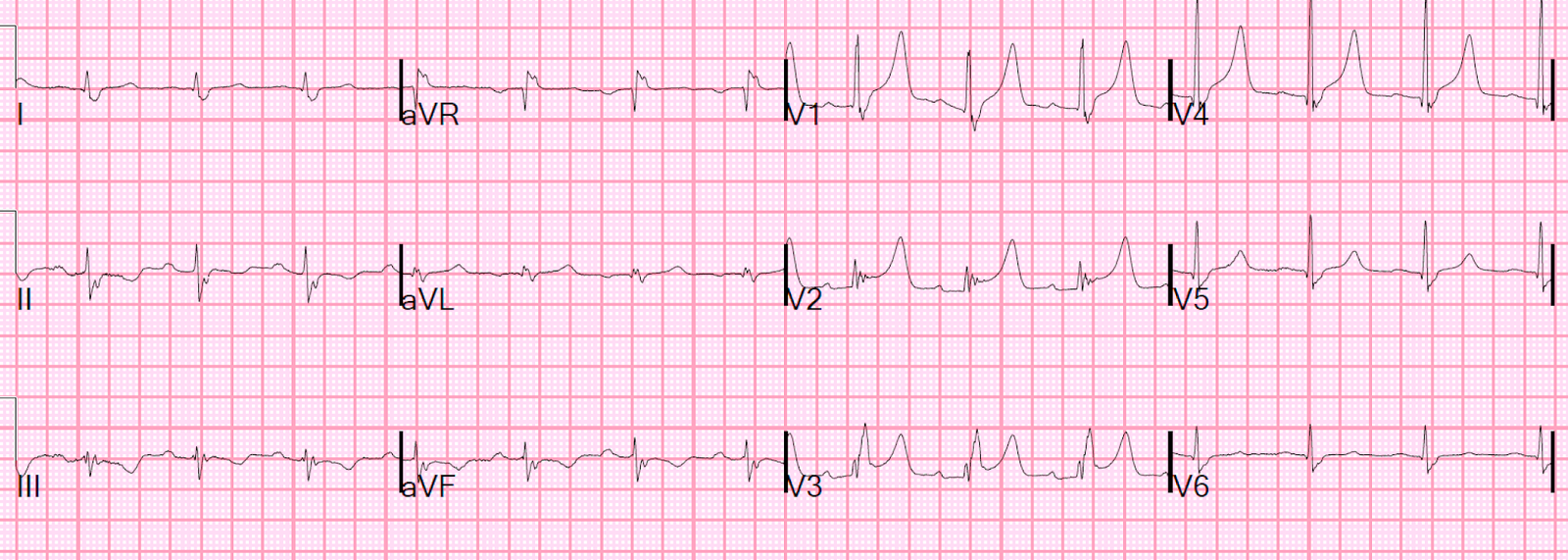
An ECG was recorded the next AM:

Less hyperacute, but still has ST Elevation in V1-V3
Formal echo with contrast:
Possible atypical stress cardiomyopathy with sparing of the apex (It looked similar to the POCUS echo)
Assessment:
Intracoronary nitroglycerin suggests a component of coronary vasospasm, LVEDP was elevated to 24. Serial troponin testing was 0.227, 0.222, 0.343, 0.393 ng/mL. TTE revealed LVEF of 40-45% and possible atypical stress cardiomyopathy with sparing of the apex. There may be some contribution of cocaine toxicity to epicardial and microvascular coronary spasm.
Apical takotsubo or “Reverse” Takotsubo. (Of course it should not be called takotsubo because that name comes from the japanese octopus trap, which implies apical ballooning with good contraction of the base.)
Read about Reverse takotsubo here:
Respiratory Failure and ST Depression: Is there Posterior STEMI?