Case 1:
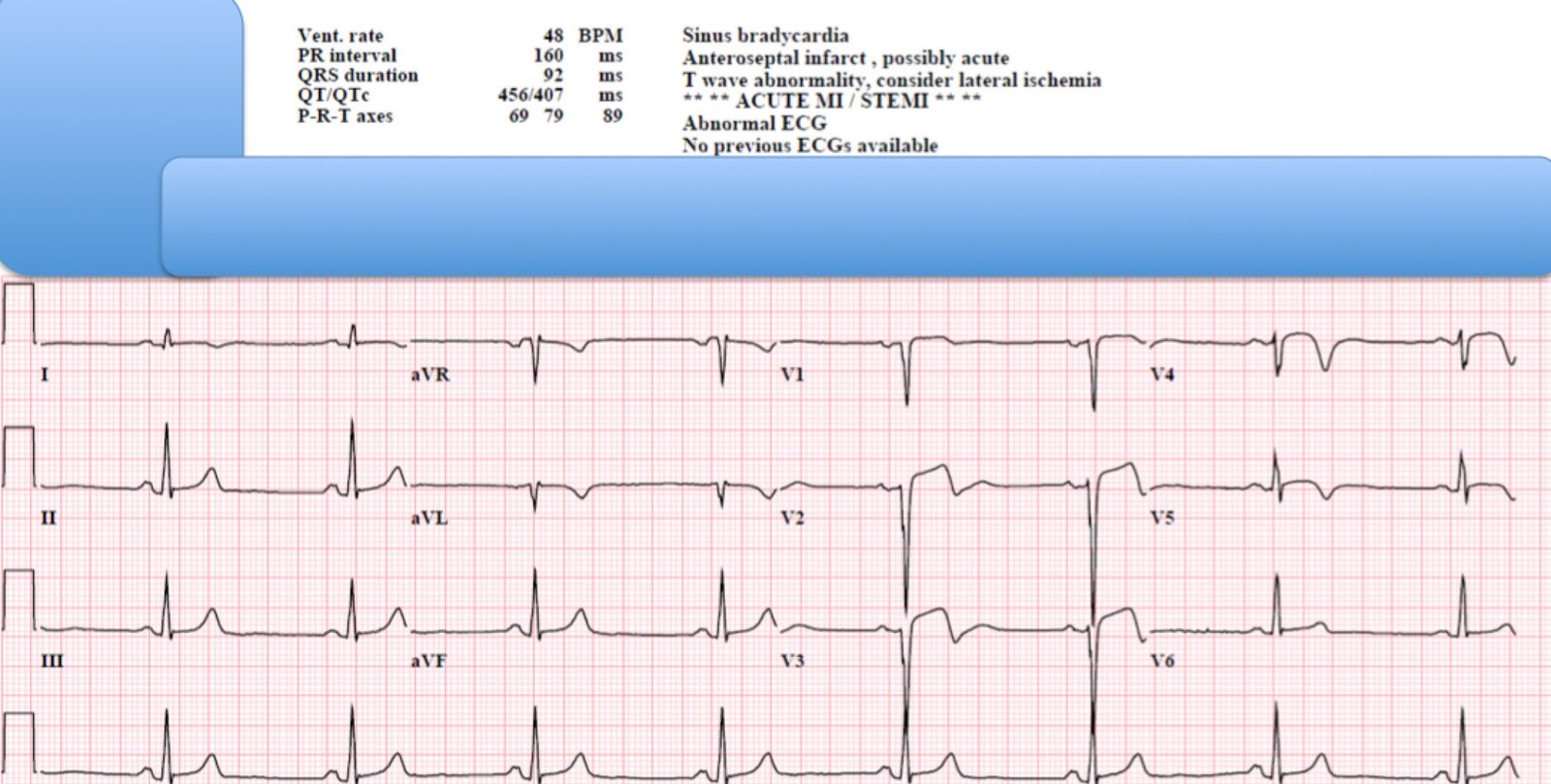
The last case had this prehospital ECG:
The Emergency Physician activated the cath lab, and it was cancelled.
 |
| Besides the obvious ST elevation and large T-waves in V2-V4.
Besides the findings in aVL and III. Notice there is no S-wave in V3. |
I gave several reasons why it must be STEMI and not Early repolarization. 3 Cardiologists said it was not STEMI.
I neglected to mention terminal QRS distortion:
This means that, in either of leads V2 or V3, there is both:
1) no S-wave AND
2) no J-wave
Early repol virtually always has at least one of these in both leads.
Case 2.
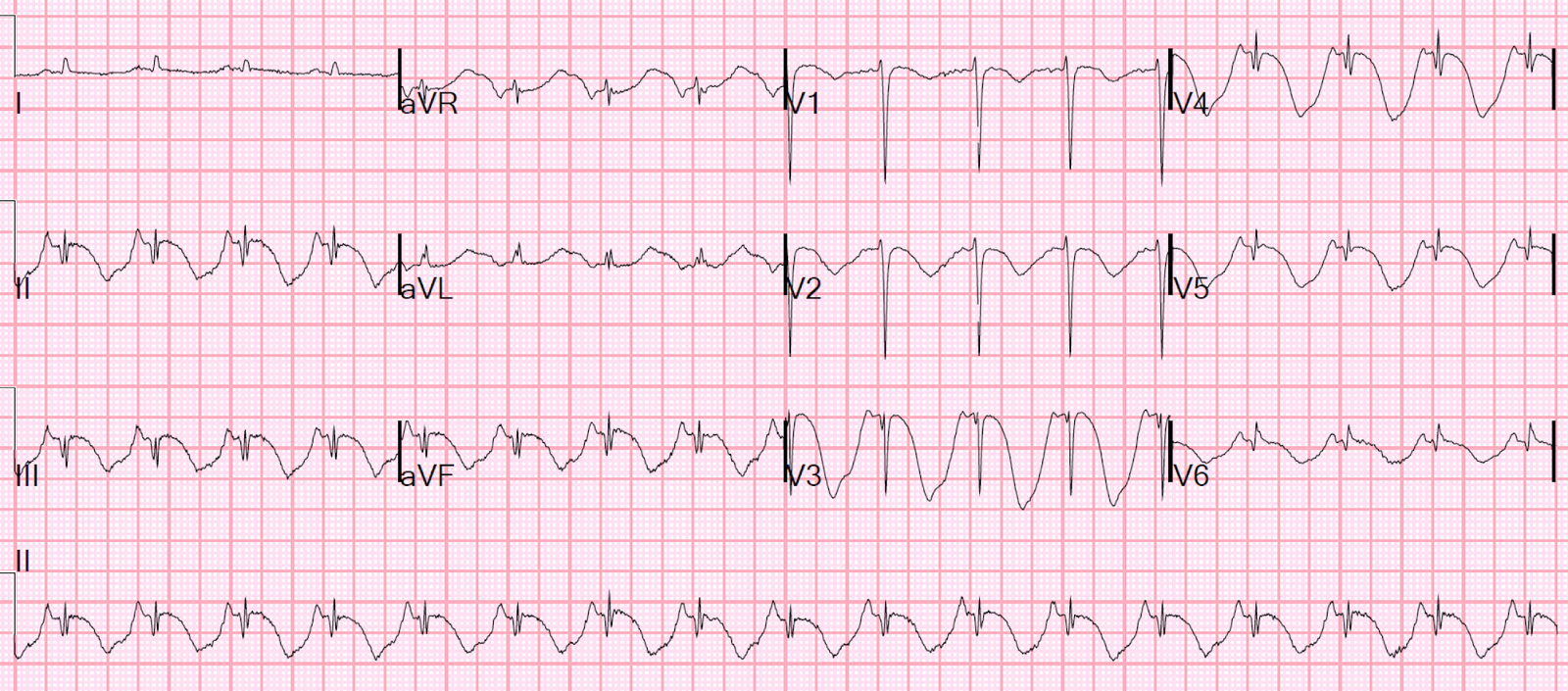
Here is a case of a 38 year old with chest pain (the full case description is here):
 |
| Notice that the end of the QRS in V3 here also does not dip below the PQ junction. Without this feature, this could easily be mistaken for early repolarization. It does not meet “critieria” for STEMI in a male under age 40 (at least 2.5 mm at the J-point in two consecutive precordial leads; here there is 2 mm in V2 and 3 mm in V3.)
This was an LAD occlusion |
I excluded cases with terminal QRS distortion from my study which produced the formula, as these were deemed “obvious” MI. In the study, 12 cases of LAD occlusion were excluded from the derivation group analysis because of terminal QRS distortion, and 24 from the validation group. So this was a common reason for the LAD occlusion to appear “obvious”.
If you use the formula in this case (which you should not because it has a feature of “obvious” MI), you get 23.36 (which is less than the cutoff of 23.4 but very close to it, and well above the “safe” cutoff of 22.0.
Case 3.
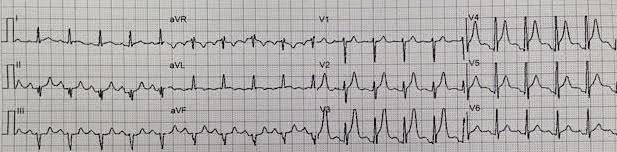
Another STEMI with Terminal QRS distortion (the full case description is here)
Here is a case which was erroneously diagnosed as pericarditis, which also should not have terminal QRS distortion:

Case 4
This is the ECG of a 50-something with Chest pain. (The full case description is here):
 |
| This one could be erroneously classified as terminal QRS distortion, but there is a J-wave in V3.
aVL and III reciprocity also falsely suggest STEMI. See how to make this subtle differentiation here. I saw this case and immediately knew it was NOT terminal QRS distortion. The patient ruled out for MI. |
Further literature:
QRS Distortion is defined as: “Emergence of the J point ≥50% of the R wave in leads with qR
configuration, or disappearance of the S wave in leads with an Rs
configuration)” (from this paper by Birnbaum). I add to this: if there are distinct J-waves in these leads, then early repolarization is still a likely possibility.