This was sent by one of our former residents.
Case
“A 40-something year old man awoke with chest pain in the middle of the night. He had a h/o HTN
and positive family history of CAD. He had no other risk factors. His pain was very typical
sounding, with nausea, diaphoresis, and SOB.”
“He was given 4 aspirin given by EMS, and was given 3 NTG and his pain went from 8/10 to 3/10. He looked a bit sick. His prehospital ECG was pretty identical to this initial ED ECG as #1. There was no prior for comparison.”
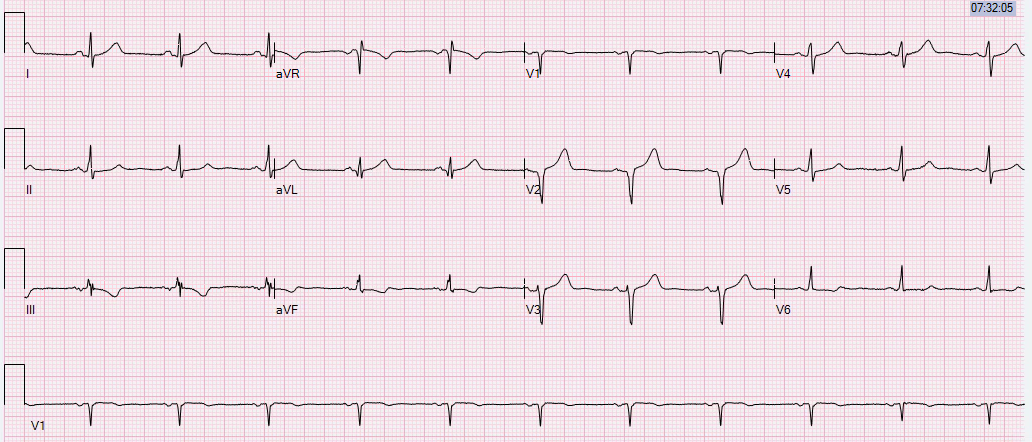
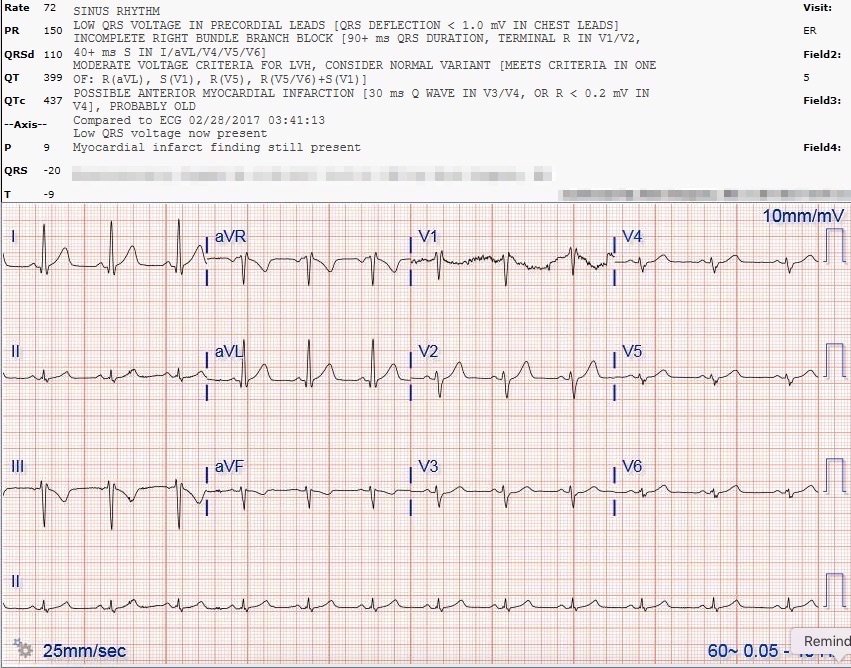
Initial ED ECG, time zero:
 |
| What do you think? |
Thoughts from the doc who sent it:
“I had a ton of concern about his T waves being too big in the lateral precordial leads.”
Smith comment: Agree! The T-waves are not large at all, but relative to the small QRS, they are indeed huge! The T-waves in I and aVL are also far too large, and have a reciprocally inverted and large T-wave in lead III. The T-wave in V2 is far too large for that small QRS.
Case continued:
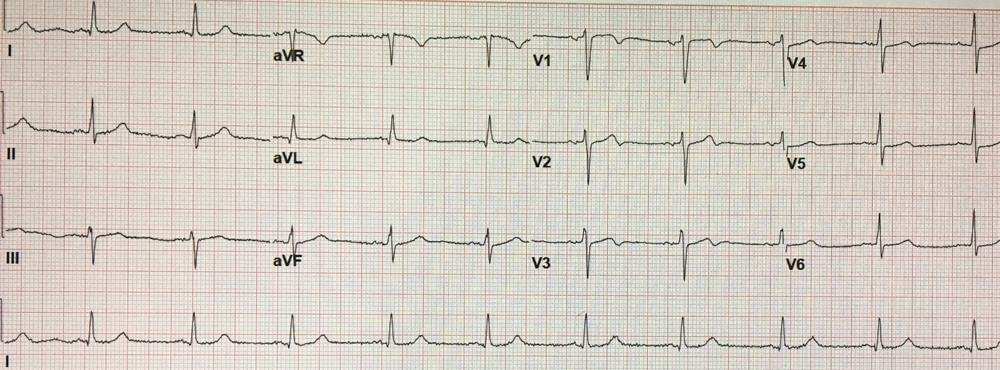
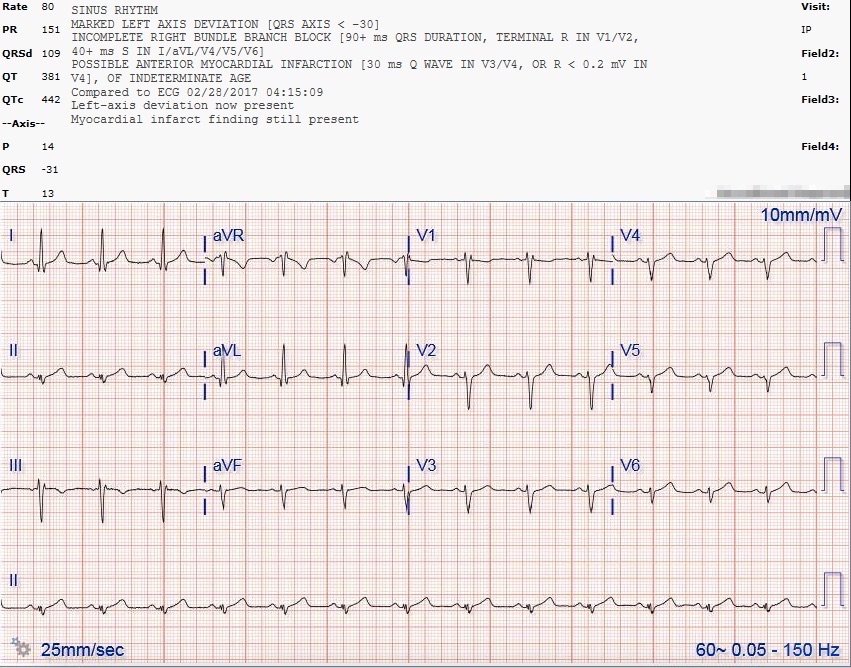
“We did a repeat ECG at about 30 minutes:”
 |
| No significant evolution, but some small resolution of T-wave size. |
“I thought it showed no significant evolution. My own bedside
echo looked to have some septal WMA (but our machines are suboptimal and
he was a little technically difficult).”
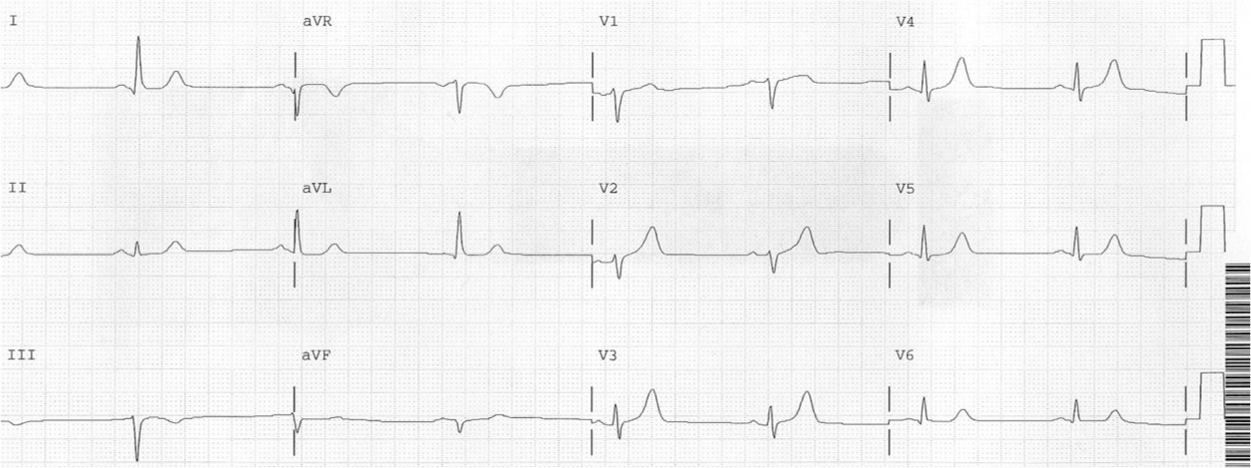
“So we did another repeat ECG:”
 |
| About the same |
“The ECG was still the same. The chest pain waxed and waned. I gave another 3 rounds of NTG with
improvement, but the pain was still there.”
“I called cardiology and told them the story. I told them very clearly of my concern for hyperacute T-waves, and the cardiologist said that this was an “overcall” and that they were
normal. Honestly, this was what I expected to hear them say.”
The initial troponin then returned at 0.080 (99% = 0.045. This slightly elevated troponin should clinch the diagnosis. However, it apparently did not change management.
It is important know that it would be very common for the initial troponin to be entirely negative, as it is in about 50% of full blown STEMI.
But the ED doc did the right thing!
“Still
concerned I called in the Echo tech in the middle of the night.”
“I sent him to the ICU on Heparin and NTG drips. About 20-30 min after admission,
I heard the cath lab announcement overhead. I look and he did in fact
have a wall motion abnormality.”
“He went to the cath lab and there was a 100% mid-LAD occlusion with thrombus and also thrombus in the posterior descending artery but this artery was open (dual culprits!). He got two stents: one in the mid LAD, restoring TIMI-3 flow, and also one in the distal
Left Posterior Descending Artery. All in all, he went to the cath lab in about 3-4 hours from
arrival.”
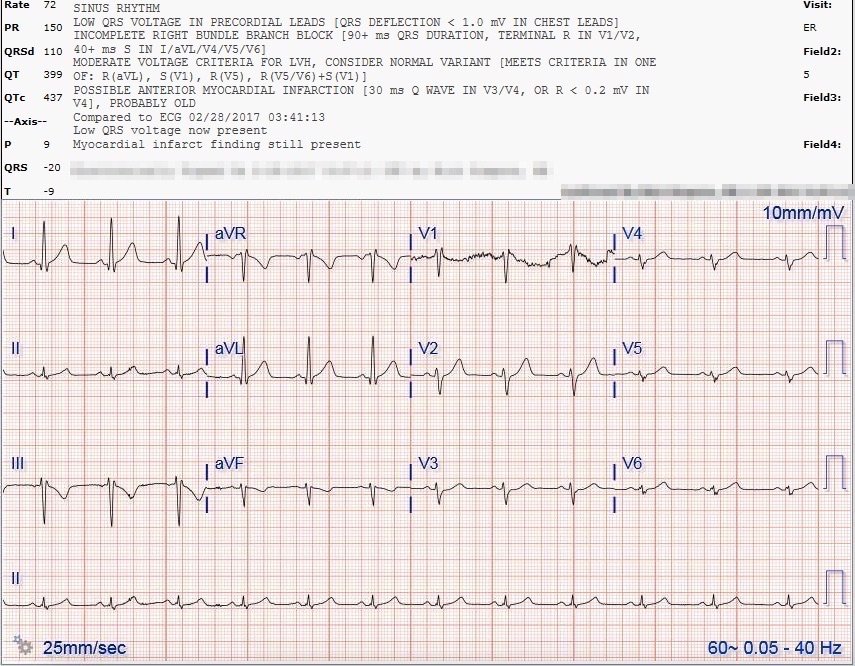
Here is the post-cath ECG:
 |
| These are normal T-waves. Note the difference!! Note that they are proportional to the small QRS!! |
Learning Points:
1. Acute LAD occlusion can be very subtle on the ECG. In a study by Marti et al., who took all patient with any suspicion of coronary occlusion to the cath lab, 13% of acute LAD occlusion had less than 1 mm of ST elevation in V2 and V3.
2. Beware hyperacute T-waves!!
3. When you are concerned about acute coronary occlusion, but the ECG is not definitely diagnostic, there is a middle way between cath lab activation and no activation: pursue agressively with diagnostic adjuncts: compare with old ECG, do serial ECGs, do high quality echo.
4. You are not held to the same Door to Balloon Time standard in these occlusions that to not meet STEMI criteria. They will be called NonSTEMIs! But these NonSTEMI patients have better outcomes with early reperfusion, compared to next day angiogram and PCI.
5. If you are concerned about subtle coronary occlusion, pursue it with formal echocardiogram
6. It is not the size of the T-wave, or the height of the ST segment, that makes the diagnosis, it is there size in proportion to the QRS!