A 30 something presented with atypical chest pain.
Here is the ECG:
 |
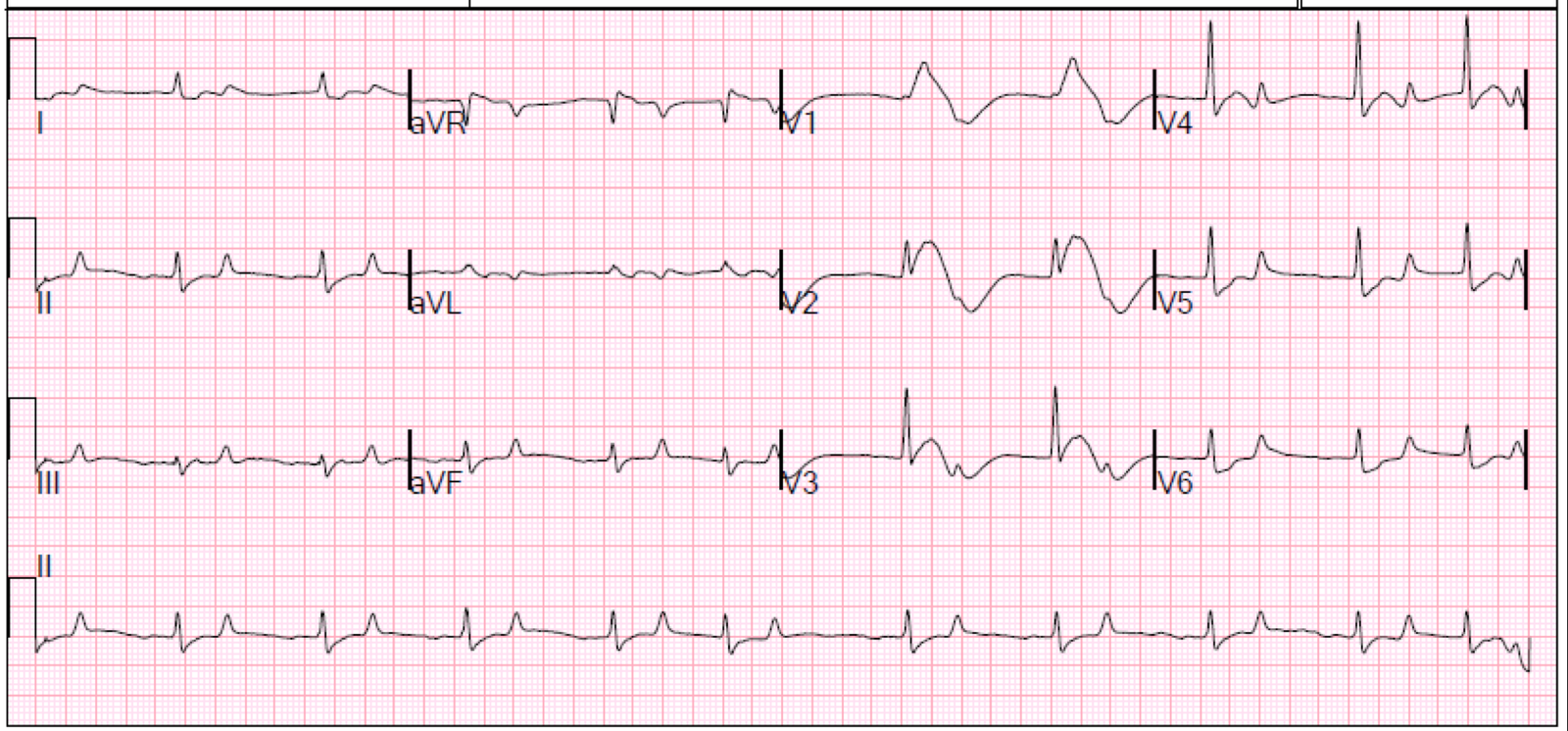
| –There is huge ST elevation in V2 and V3, approximately 5 mm.
–There is some ST elevation in aVL with some minimal reciprocal ST depression in III –There is a small q-wave in V4. –There are also large S-waves in I and II, and a large R-wave in V1, suggesting right ventricular hypertrophy |
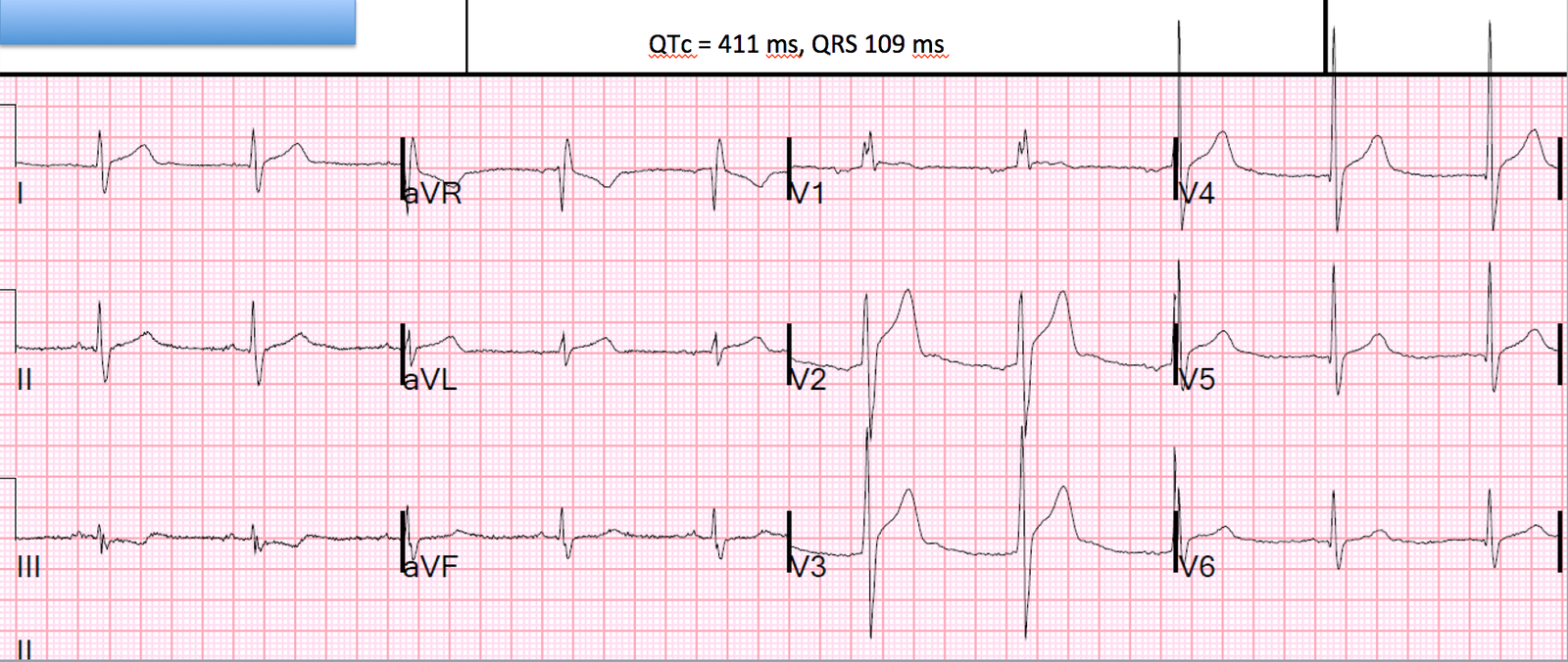
It is risky to apply the early repol vs. LAD occlusion formula when there are other indications that this may be MI, such as 1) Q-wave in V4 and 2) STE in aVL with STD in III. However, when I saw this (I did not take care of the patient), I thought this “looked” like early repol, and I did apply the formula:
STE 60 V3 = 5 mm
QTc = 411 ms
R-wave amplitude in V4 = 25 mm
Formula value = 22.079. This is very low. Less than 22 is about 97% sensitive for LAD occlusion.
This is very low. Serial ECGs were recorded and they remained the same. The patient ruled out for MI and all ECGs were stable.
Unfortunately, no echo was done to assess for RV hypertrophy.
Learning Points
1. Early repolarization can have Scary ST elevation
2. Pretest Probability is Critical. Here, the low pretest probability was an important factor in this decision: in a young patient with atypical pain, scary ST elevation is much less likely to be due to ischemia.