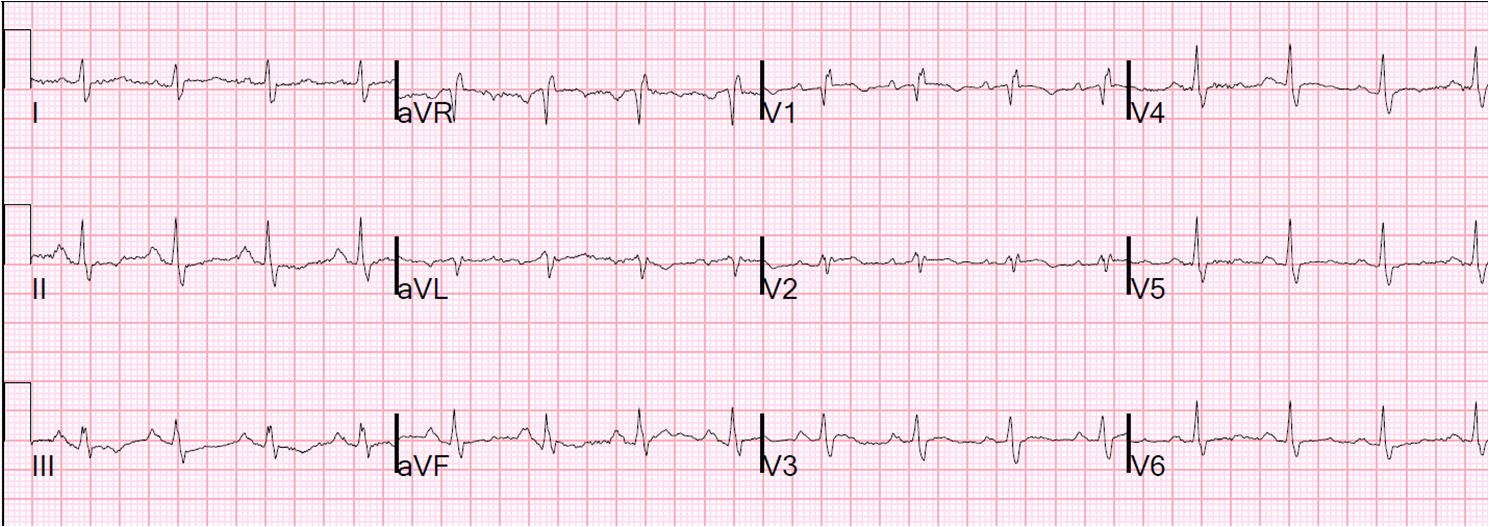
A woman in her 60s presented with a COPD exacerbation. She also complained of some sharp chest pain with coughing. She was in moderate distress consistent with a moderate COPD exacerbation. An ECG was recorded:
 |
| The computer reading was: “Anterior ST elevation due to early repolarization.” |
The treating physicians were alarmed by the first ECG due to the
apparent hyperacute T-wave in V3. They applied the LAD occlusion vs.
early repol formula (see sidebar for excel applet and see previous posts),
using computerized QTc of 416, STE60V3 of 3.0 (it may be 3.5) and R
amplitude in V4 of 13, and found a value of 23.9 which is greater than
23.4 and indicates LAD occlusion.
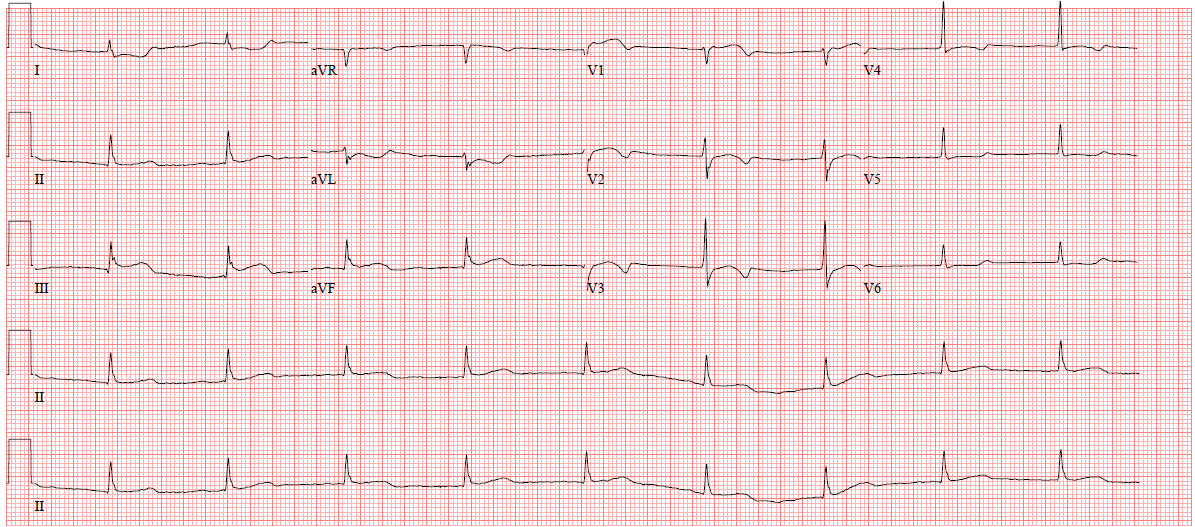
So they sought out a previous ECG:
Here is one from 2 weeks prior:
 |
| What do you think? |
Now they were even more worried, as the acute ECG is much different. However, this patient did not have chest pain that was in any way typical. They were appropriately reluctant to activate the cath lab, but did call the cardiologist, who was also appropriately worried.
A bedside ED cardiac echo was done during the evaluation:
The embed code has stopped working consistently. You can see the video by clicking here:
First bedside ultrasound, subcostal view from Stephen Smith on Vimeo.
Here is an annotated still picture of one frame from above:
 |
| The blue arrow points toward the tricuspic valve and the base of the RV. The red arrow points toward the mitral valve and the base of the LV |
Second ultrasound, apical view from Stephen Smith on Vimeo.
What do these cardiac echo clips show?
First video clip: This clearly shows the bases of both the right and left ventricles are beating vigorously, but the apex is hardly moving at all.
Second clip: It is easy to see the base of the heart contracting, but although the
image quality of the apex is poor, one does not see much motion there
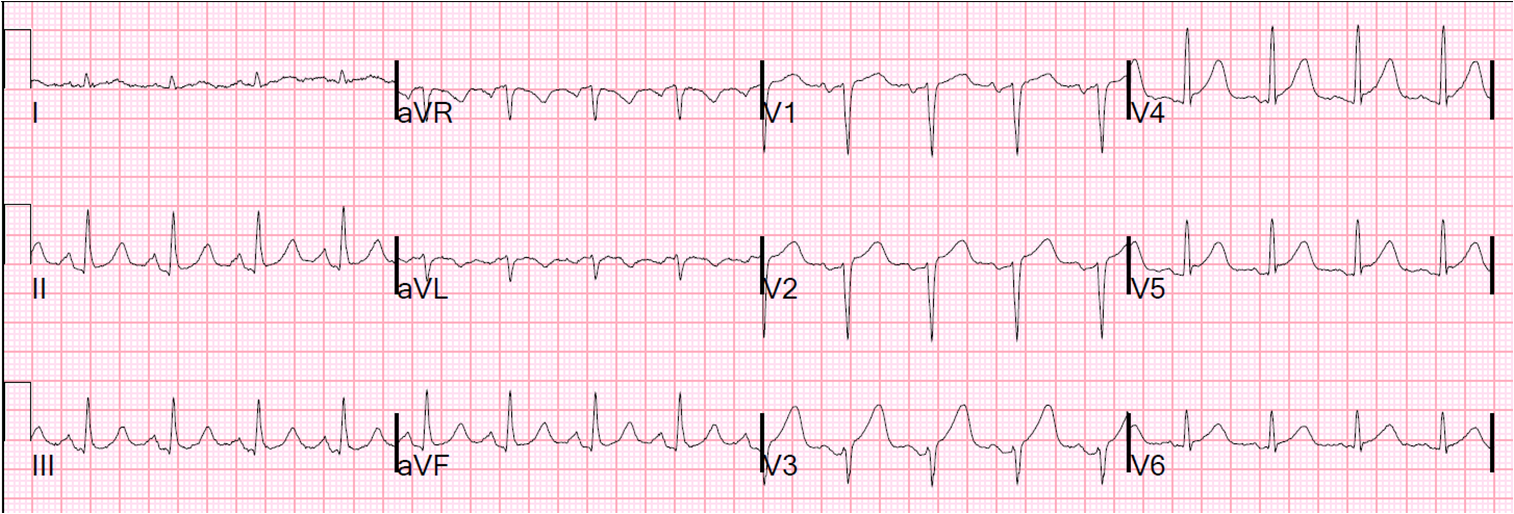
At this point, the patient started having crushing chest pain and another ECG was recorded:
 |
| Now there is increased ST elevation in V3. See outcome below. |
A formal ultrasound with Definity contrast was being done at approximately the same time as the onset of severe chest pain. It showed:
–Regional wall motion abnormality-distal septum anterior and apex akinetic, large.
–Regional wall motion abnormality-distal inferior wall akinetic.
–Regional wall motion abnormality-lateral akinetic.
–There good contractility of the base of the heart.
–Normal left ventricular size.
—Decreased right ventricular systolic performance severe.
–Regional wall motion abnormality-right ventricle .
Outcome
This ultrasound and the bedside ultrasounds show “apical ballooning”, all highly suggestive of Takotsubo stress cardiomyopathy (which is likely to accompany a stressful event such as a COPD exacerbation), but it is also compatible with acute LAD occlusion. The crushing chest pain, wall motion abnormalities, hyperacute T-waves and ST elevation were possibly due to takotsubo stress cardiomyopathy but also possibly due to LAD occlusion. The patient was taken to the cath lab and had no obstructive LAD lesion and no culprit. The troponin I peaked around 1.5 ng/ml.
Can one distinguish on the ECG between takotsubo stress cardiomyopathy (SCM) and acute STEMI??? Not reliably! There are some ECGs that are clearly due to stress cardiomyopathy (widespread T-wave inversion). But when the ECG is recorded during the ST elevation phase, I know of no reliable way to differentiate these. I reviewed this topic in this post. To sum it up very briefly, if it appears to be an infero-antero-lateral STEMI, it is more likely to be SCM than if the ST elevation is in one coronary distribution (e.g., anterior, as in this case); however, again, this is not more than 80% reliable. The cellular pathophysiology of SCM is identical to STEMI (severe transmural ischemia), but it is due to catecholamine stress and small vessel constriction (NOT due to epicardial coronary flow obstruction); and that is why the ECG is nearly identical.
Here are several more cases of SCM.
Does cardiac ultrasound definitively differentiate the two entities? In the acute phase, apical ballooning is highly suspicious for SCM, but large wall motion abnormalities may also be seen in patients with proximal LAD occlusion in a type III (wraparound) vessel, affecting anterior, lateral, and inferior walls. These STEMI cases also have widespread ST elevation as in SCM.
Is the Right Ventricle involved in Takotsubo Stress Cardiomyopathy?
RV SCM has been described, appears to accompany LV takotsubo cardiomyopathy up to 25% of the time and be associated with worse LV function. See this article: and also this article:
http://content.onlinejacc.org/article.aspx?articleid=1142735
Lesson:
There is no more vexing ECG mimic of acute STEMI than SCM because the underlying cellular pathophysiology is the same. It is unusual to make the diagnosis without an angiogram.