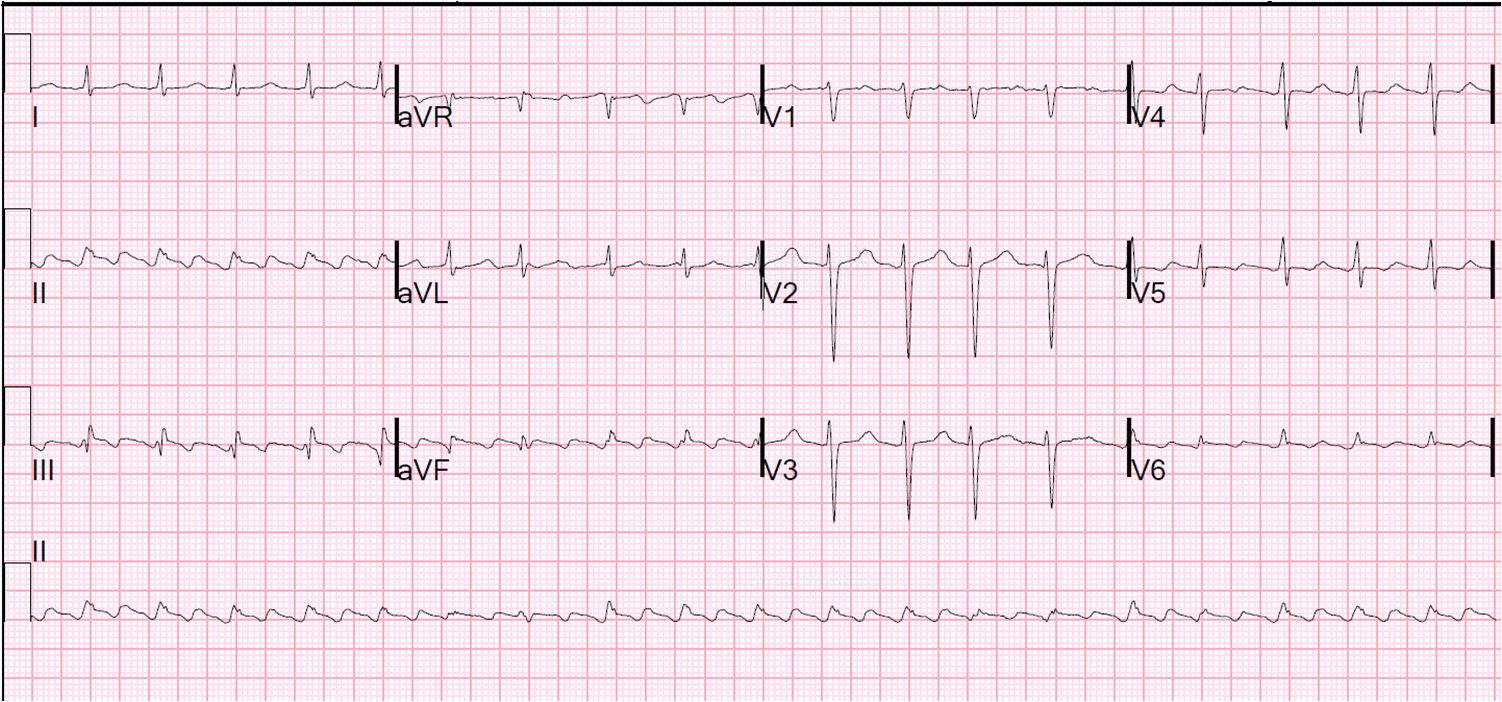
A male in his 30’s presented with chest pain. Here is his initial ECG:
 |
|
So, the only plausible reasons for ST elevation are anterior STEMI or
Early Repolarization. One might be tempted to apply the formula that
helps to differentiate the two. However, when we studied these ECGs, we excluded patients with features that made STEMI “obvious,” or at least not subtle. These features included Q-waves and Terminal QRS distortion. In this case, the Q-waves do not make it an obvious MI, but the QRS distortion does:
QRS Distortion is defined as: “Emergence of the J point ≥50% of the R wave in leads with qR
configuration, or disappearance of the S wave in leads with an Rs
configuration)” (from this paper by Birnbaum). I would add to this: if there are distinct J-waves in these leads, then early repolarization is still a likely possibility. In this case, there are no distinct J-waves in V2 or V3 (although there is a small one in V4)
Thus, this should be thought of as diagnostic of anterior STEMI. If the formula had been used, then the
value would have been [1.196 x 3.5]+[0.059 x 402]–[0.326 x 17] = 22.362 (which is less than 23.4 and thus consistent with early repolarization). The formula would have given a false negative, because this was an LAD occlusion.
Learning Point:
When there is Terminal QRS distortion (absence of BOTH an S-wave and a J-wave in EITHER of leads V2 or V3, it is not early repolarization. When the differential diagnosis only includes early repol and LAD occlusion, then LAD occlusion is strongly favored.