This was sent by a former resident.
A 30-something male presented 4 hours after onset of chest pain. He had had some chest pain 2 days earlier that resolved on its own. He complained of nausea and dyspnea also.
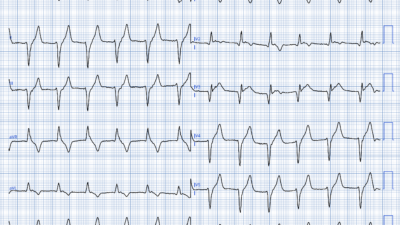
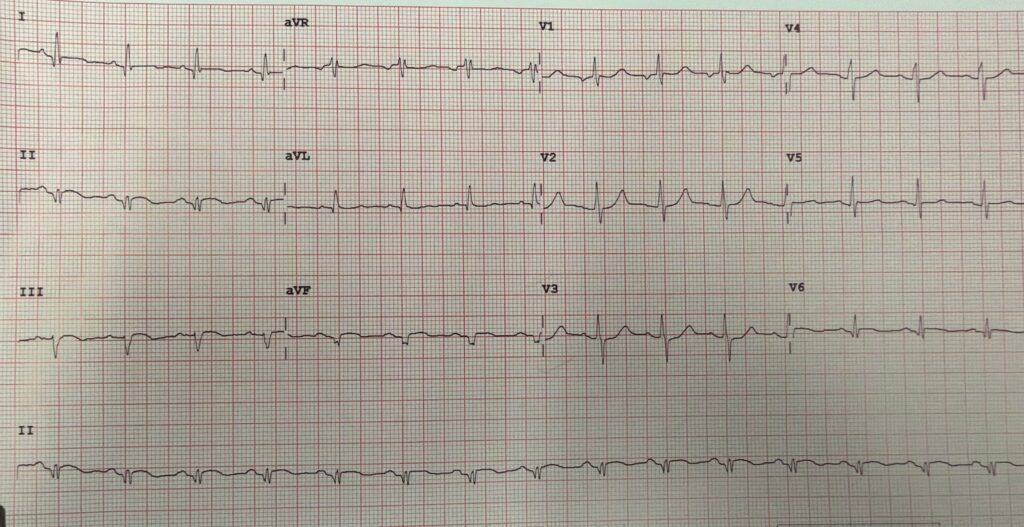
Here is his ED ECG:
What do you think?
For readers of the blog, this should be an easy one, even though young patients are often dismissed:
There is slight STE in leads II, III, and aVF, and slight reciprocal ST depression in aVL (Diagnostic of inferior OMI). There is ST depression in leads V3 and V4 (diagnostic of posterior OMI). There is slight STE in lead V6, which is on the way around to the posterior wall (diagnostic of lateral OMI)
So there is inferior, posterior, lateral OMI.
My former resident activated the cath lab.
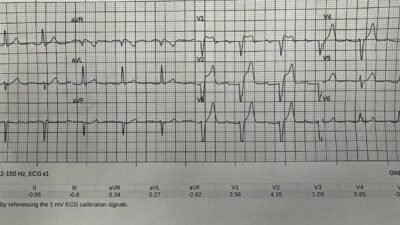
Here is the Queen of Hearts interpretation:
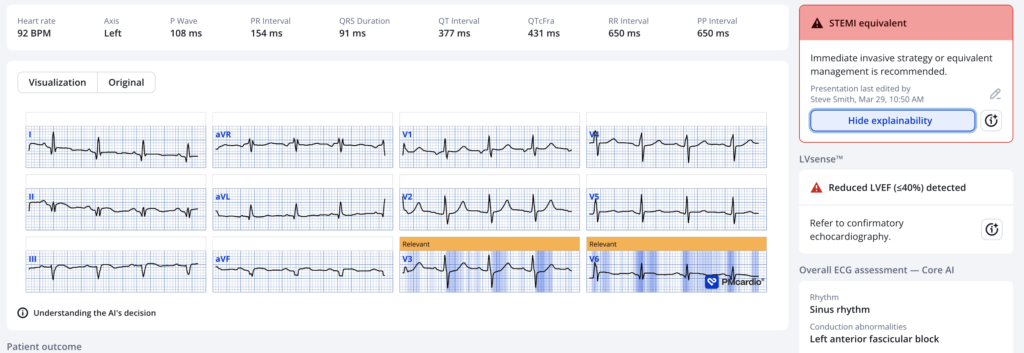
Interestingly, she does not comment on the inferior leads, only posterior and lateral.
Angiogram
The cath report says: “Inferoposterior STEMI s/p successful aspiration and mechanical thrombectomy followed by PTCA with restoration of TIMI-3 flow. Severe coronary disease including LAD CTO with right to left collaterals, subtotally occluded diagonal, proximal ramus and focal rPLV disease. Cangrelor drip as bridge to Bypass consideration”.
Wow, nasty report. He does not tell us which artery had PTCA. Could be either RCA or Circ, probably Circ because if the LAD is supplied by right to left collaterals and there was occlusion of the RCA, there would have been LAD territory OMI.
Troponin I rose to at least 43,000 ng/L (large infarct)
No echo was available.
Learning Points:
- A very large infarction, with occlusion, and severe coronary disease, can occur in a young patient without any lead manifesting the “STEMI Diagnostic criteria”.
- Cardiologists frequently call a case a “STEMI” if there is occlusion regardless of the absence of ST Elevation. (We have found that the single most important factor in the Diagnosis of STEMI vs. NSTEMI is time to intervention, regardless of STEMI criteria or presence of occlusion!!)
de Alencar JN, Meyers H, Frick WH, McLaren JTT, Smith SW. Door-to-balloon time outperforms ST-segment elevation in predicting the STEMI vs. NSTEMI final diagnosis. J Clin Med [Internet] 2025;14(18):6588. Available from: http://dx.doi.org/10.3390/jcm14186588
- See more cases of YOUNG patients.
= = =
======================================
MY Comment, by KEN GRAUER, MD (3/30/2026):
Today’s case makes for a superb “short-and-sweet” consolidation of KEY concepts regarding many of the clinical essentials of acute OMI. The excellent Learning Points by Dr. Smith are worthy of repetition:
- — i) A very large MI (with acute coronary occlusion and severe underlying coronary disease) — can occur in a surprisingly young patient, even without ECG criteria for a STEMI.
- — ii) The single most important factor regarding distinction between a “STEMI” vs a “NSTEMI” — is the time until intervention (which is especially likely to be delayed in those cases in which “NSTEMI” is the label used to describe the event).
= = =
KEY Points highlighted by Today’s CASE:
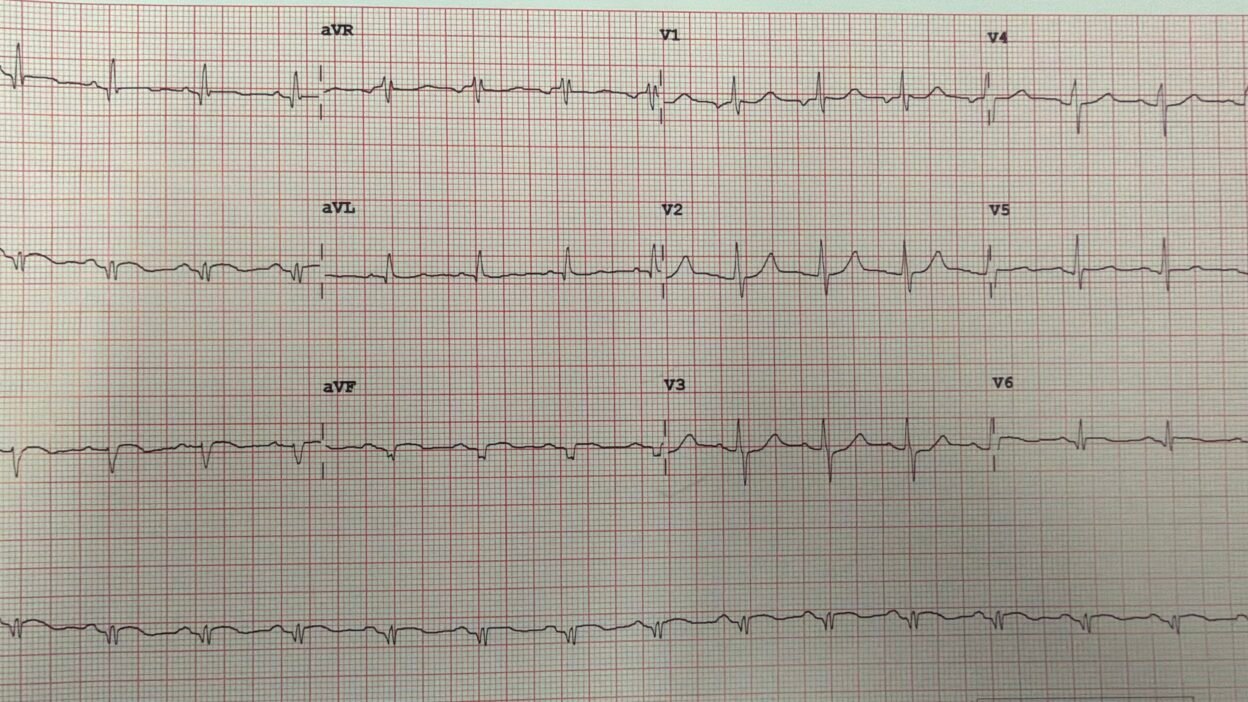
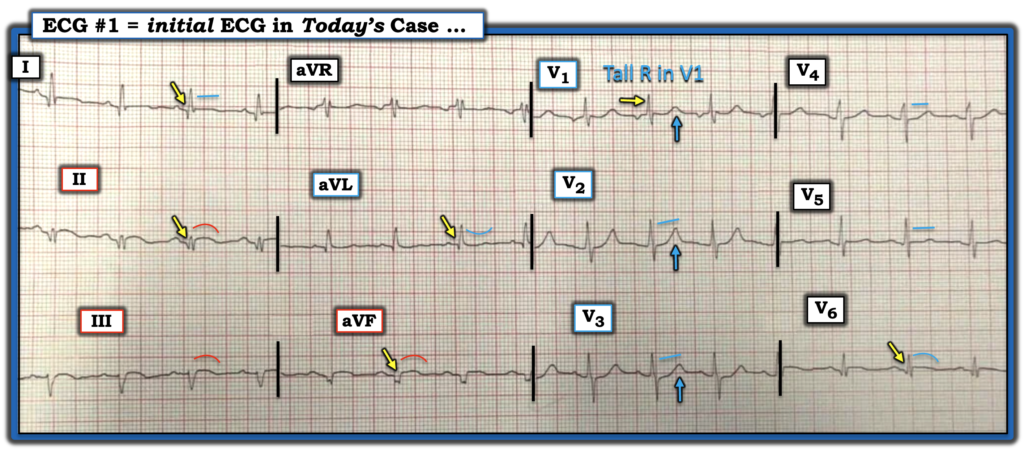
For clarity in Figure-1 — I’ve labeled today’s ECG:
- Correlating the History to the initial ECG shown in Figure-1 is insightful — and helps to explain the ECG findings. Today’s patient had CP (Chest Pain) that began and resolved ~2 days earlier. The patient’s CP then recurred 2 days later, with him presenting to the ED ~4 hours after that.
- This history is consistent with recent infarction, perhaps occurring ~2 days earlier (ie, at the time of the initial CP episode). The patient’s CP recurrence could reflect reclosure of the culprit artery — or — given multi-vessel involvement that becomes evident on cardiac cath, this recurrence of CP could reflect spread in the extent of involvement from alterations in collateral flow.
= = =
ECG Findings in Figure-1:
- Multi-vessel disease is suggested in Figure-1 — by the finding that virtually all leads show ST-T wave abnormalities.
- YELLOW arrows in no less than 5 leads highlight Q waves that are likely to be “pathologic” (ie, likely to indicate infarction at some point in time). Although the Q waves in lateral leads I, aVL and V6 are not overly deep or wide — in view of the small size of the QRS in these 3 leads, I interpreted these Q waves as at least potentially pathologic.
- That said — the Q waves in leads II and aVF are clearly pathologic (ie, given relative width of the Q wave and tiny size of the QRS in lead II — and — given the notched [fragmented] QS morphology in lead aVF).
- As per Dr. Smith — ST segment coving with slight elevation in each of the inferior leads (= leads II,III,aVF) — in association with the mirror-image opposite picture of reciprocal ST depression in lead aVL — is diagnostic of inferior OMI at some point (likely within the past 2 days given the history).
- In the chest leads — the Tall R wave in lead V1 is a Q-wave “equivalent” for posterior MI — with ST segment straightening in lead V2 (instead of the slight upsloping ST elevation that is normally seen) — and both straightening and slight ST depression in leads V3,V4 — being diagnostic of posterior OMI. Putting these findings together — I thought the Q wave equivalent ( = predominant R wave) in lead V1 + the prominent positive T waves (BLUE arrows in leads V1,V2,V3) were most consistent with some degree of spontaneous reperfusion (presumably from the CP episode that spontaneously resolved 2 days earlier).
- Finally — ST segment straightening in leads I,V5 — and subtle ST segment coving in lead V6 complete the picture of multi-lead involvement from underlying multi-vessel disease.
- NOTE: We are not told anything about this patient’s prior history. That said — the ECG in Figure-1, and the cath findings reported above in this 30-year old — counter the common perception that younger patients are not supposed to have large acute infarctions with extensive underlying coronary disease.
= = =
Figure-1: I’ve labeled today’s ECG.
= = =
= = =
= = =