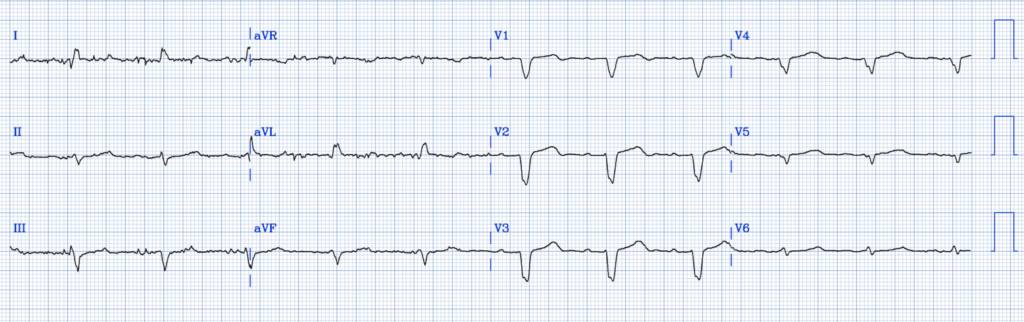
A middle-aged male presented with chest pain, onset 1 hour prior. He had an ECG recorded immediately:
What do you think?
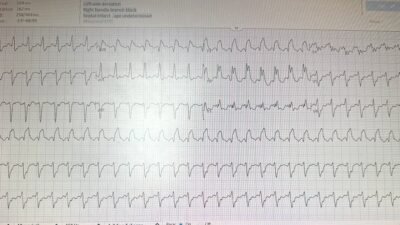
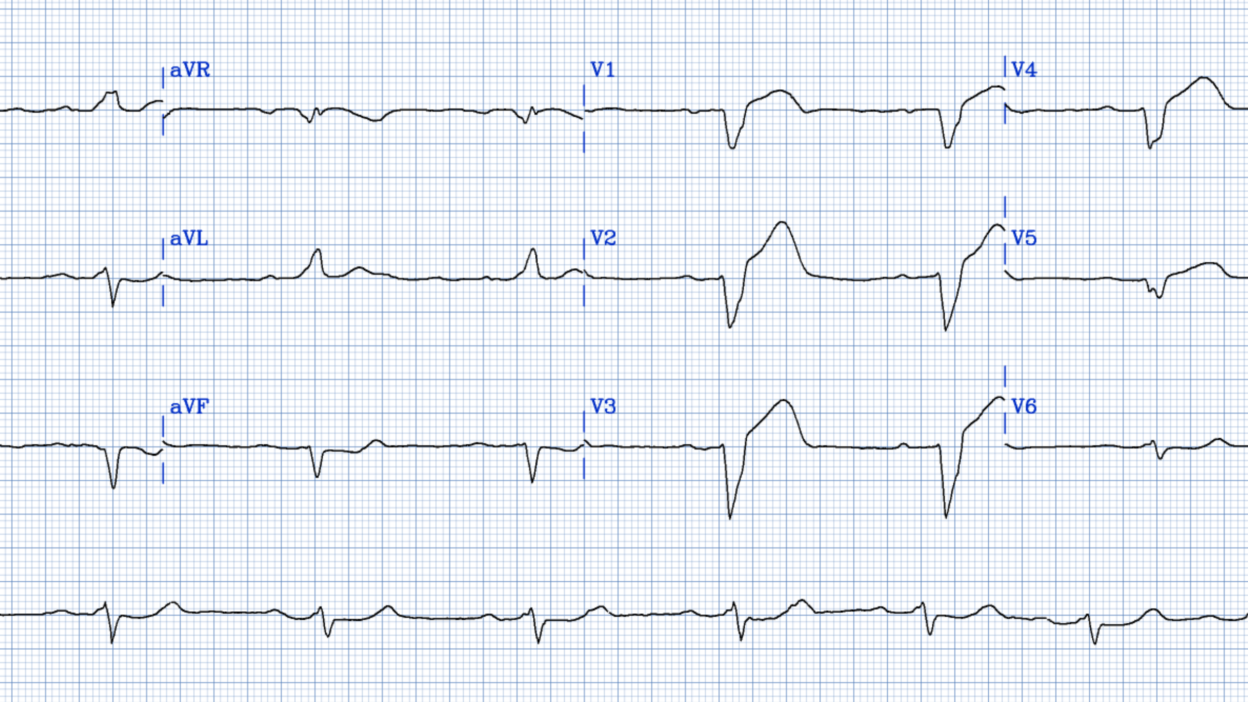
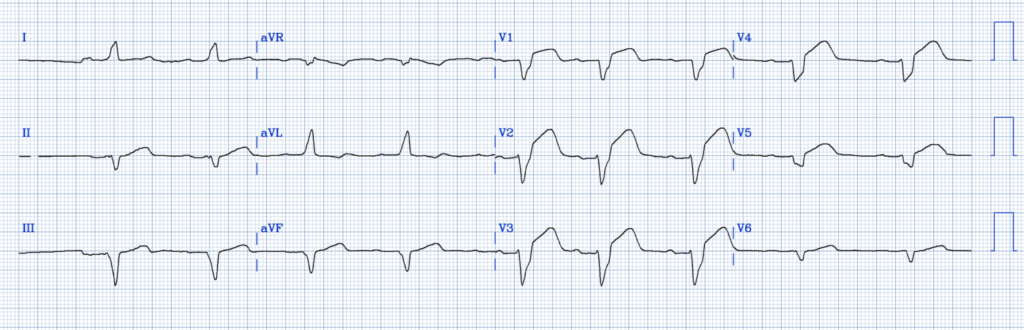
There is sinus with a wide complex that is left bundle branch block (LBBB). There is also proportionally excessively discordant ST Elevation in lead V2, and hyperacute T-waves in leads V1-V4. By the Smith Modified Sgarbossa criteria, one need have only 1 lead with proportionally excessively discordant STE [ST/S ratio of 25% (80% sensitive and 99% specific)]. [ST/S ratio, with ST measured at the J-point relative to the PQ junction/QRS onset]. An ST/S ratio of >/= 20% is 84% sensitive and 94% specific. I get worried about any ratio > 15%, as the normal maximal ratio of ST/S in V1-V4 is 11%.
The ratio in V2 is 2.75/7.5 which is 37%.
Whether the LBBB is new or old does not matter! Alencar JN de, et al. Accuracy of Left Bundle Branch Block Chronology and Electrocardiography Criteria for Acute Myocardial Infarction Diagnosis: A Systematic Review and Meta-analysis. Arq Bras Cardiol [Internet] 2025;122(10):e20250109. Available from: http://dx.doi.org/10.36660/abc.20250109.
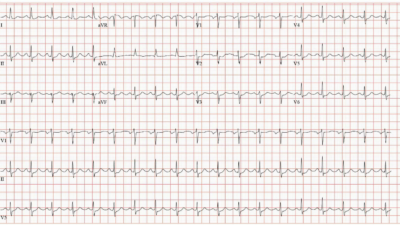
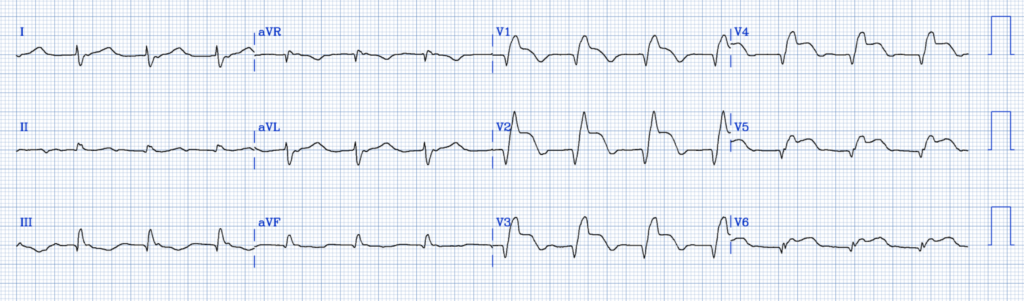
So this ECG is diagnostic of LAD occlusion. For reference, here is an example of LBBB that has no ischemia (and of course no OMI):
Here they are side by side:
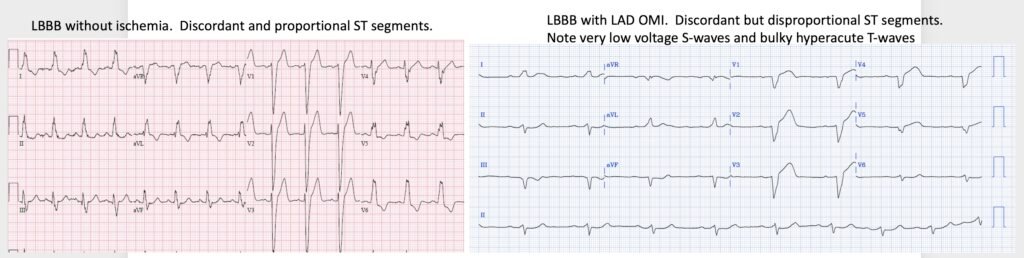
All ST segments are discordant AND proportional.
Here is what the PMCardio Queen of Hearts AI ECG Model says:

New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical). As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: Certain AI ECG Modules are CE-marked medical devices under EU MDR and are certified for marketing only in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA, and is not yet available in the USA.
Unfortunately, the providers did not make the diagnosis.
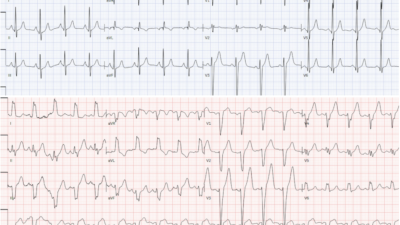
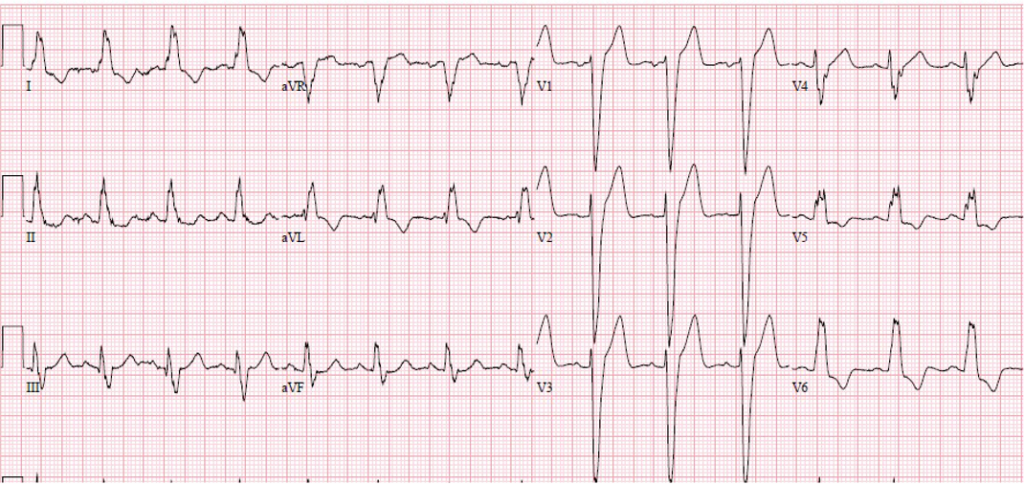
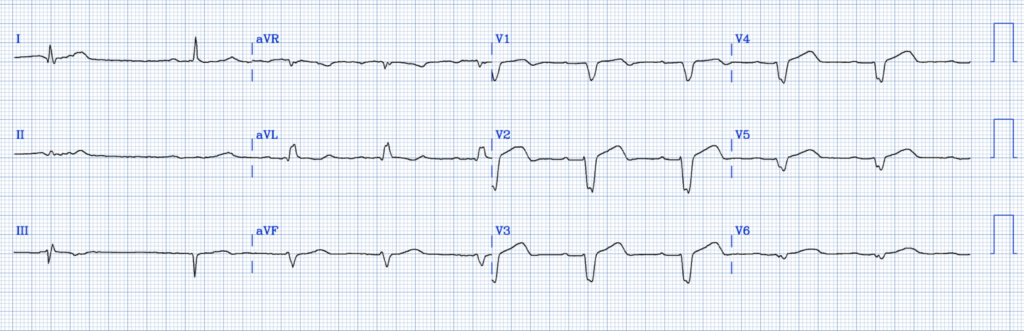
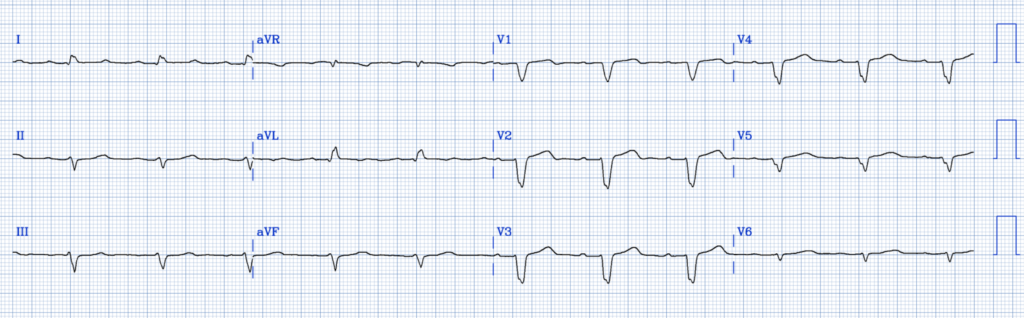
They recorded another ECG 1 hour later:
Now, there is far more ST Elevation: 1.75 mm in V1, 3.5 mm in V2, 2.5 in V3, 1.5 in V4, with ratios of 35%, 50%, 25%, and 28%. (Now there are 4 ratios greater than 25%!)
The cath lab was activated and a 100% LAD Occlusion was found. Troponin I peaked at a massive 270,000 ng/L, indicative of a huge amount of myocardial loss.
Unfortunately, an enormous amount of myocardium died in the one hour delay. The patient could have had reperfusion at 2 hours post onset, but instead it was at 3 hours post onset. Remember, 80% of the mortality benefit of reperfusion occurs in the first 4 hours after chest pain onset. See how much benefit is lost by delaying by 1 hour. From hour 2 to hour 3, 30% of the mortality benefit is lost (see this graph):
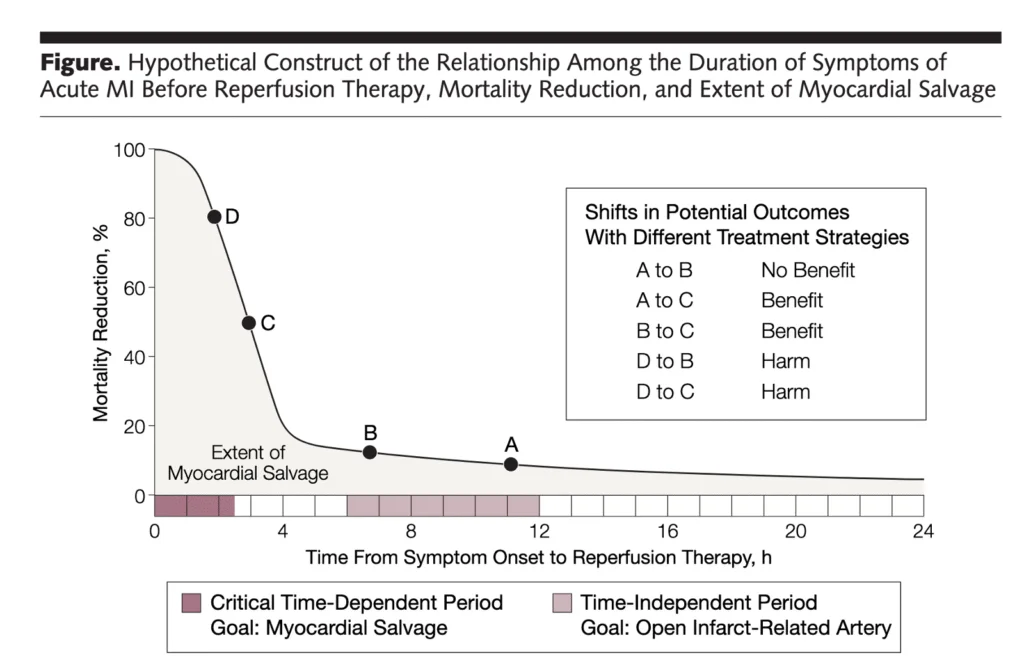
Gersh BJ, Stone GW, White HD, Holmes DR Jr. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the shape of the future? JAMA [Internet] 2005;293(8):979–86. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15728169Here are subsequent ECGs
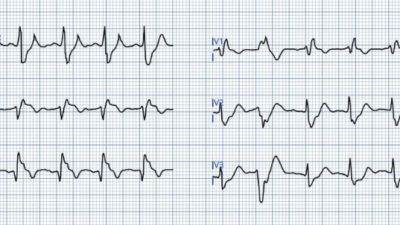
This is 20 minutes after PCI:
This now shows the reperfusion rhythm AIVR. (notice there are no P-waves). The ventricular rhythm starts from the LV, resulting in a Right Bundle Branch block (RBBB) morphology. AIVR is a reperfusion rhythm. It shows persistent ST Elevation and makes the OMI much more recognizable, even though it is reperfusing, with terminal T-wave inversion.
See this case: Probable Left Main coronary artery occlusion/obstruction, with STE in aVR, alternating BBB, and arrest
Here is 2.7 hours after PCI:
AT 5.7 hours after PCI:
And now at 9.5 hours after PCI:
OMI is very often missed in LBBB, but need not be. I have many other such cases on this blog; here is one incredible miss: Acute chest pain with LBBB and obvious OMI, worsening on serial ECGs, but repeatedly missed by physicians and Marquette 12SL
Learning Points:
- Use the PMCardio Queen of Hearts AI ECG Model on EVERY ECG so you don’t miss an OMI.
- The Smith Modified Sgarbossa criteria work. They are recommended by nearly all Cardiology guidelines for diagnosis of acute coronary occlusion in the presence of LBBB.
= = =
==================================
MY Comment, by KEN GRAUER, MD (5/11/2026):
The management in today’s post is problematic for a number of reasons. I focus My Comment on the initial ECG — as this is where the problems begin.
- — i) Despite ST-T wave abnormalities in virtually every lead — the acute findings were not recognized by the provider team.
- — ii) I suspect that the provider team did not recognize the conduction defect. This is relevant — because criteria for acute ischemia/infarction vary depending on conduction properties.
- — iii) Despite the history of acute CP (Chest Pain) and the uncertainty about how to interpret ECG #1 — the initial ECG was not repeated for 1 hour. As we have shown in numerous cases in Dr. Smith’s ECG Blog — ”dynamic” ST-T wave changes can develop within minutes in an actively evolving infarction. Given how high the peak Troponin eventually rose to ( = 270,000 ng/L) — and — Given how much the ECG changed by the time the initial ECG was finally repeated 1 hour later — it seems highly likely that significant ST-T wave changes would have been noted had the initial ECG been repeated much sooner (ie, ideally within 10-20 minutes after the initial tracing whenever any uncertainty exists about whether an OMI is actively evolving).
Bottom Line: As per Dr. Smith — the fastest and easiest way to recruit help at the bedside to assist when assessing for acute ischemia/infarction — is to routinely use the PMcardio Queen of Hearts AI ECG Model on every patient who presents to the ED with new symptoms potentially due to acute MI.
- Feedback to providers on cases like this is essential — as is the equally tough and humbling work of learning what was missed on the ECG — and how not to miss it the next time (ie, understanding which leads and what ST-T wave findings enabled QOH to instantly identify the acute OMI that providers overlooked).
= = =
Another Look at Today’s Initial ECG …
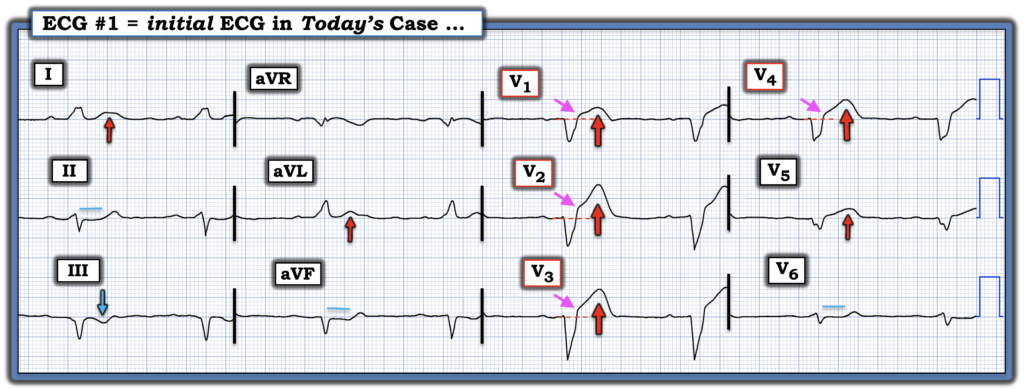
I’ve reproduced and labeled today’s initial ECG in Figure-1. As per Dr. Smith’s above discussion — modified-Smith-Sgarbossa criteria that are diagnostic of acute LAD occlusion are clearly satisfied. That said — it’s worth citing the gamut of ECG abnormalities that should be noted.
- The rhythm is sinus bradycardia, at a rate a bit below 50/minute (the R-R interval being a bit over 6 large boxes in duration). This degree of bradycardia in an acute CP patient should immediately heighten concern.
- There is 1st-degree AV Block (PR interval ~0.24 second).
- The QRS is wide (Clearly ≥3 large boxes ==> at least 0.12 second in duration in multiple leads). As per Dr. Smith — QRS morphology is most consistent with LBBB (Left Bundle Branch Block), in that there are all upright QRS complexes in left-sided leads I and aVL — and predominantly negative complexes in the anterior leads (albeit as per my “P.S.” below — there is nowhere near the positive R wave typically seen in lead V6 with true LBBB).
- There is low voltage (ie, No QRS complex in the 6 limb leads is >5mm — with dramatically reduced QRS amplitude in lateral chest leads V4,V5,V6). It’s important to remember that in a patient with acute CP — among the causes of low voltage is extensive infarction with reduced cardiac output from myocardial “stunning” (CLICK HERE — for the LINK at the top of every page in Dr. Smith’s ECG Blog to our List for the Causes of Low Voltage).
In addition to satisfying modified-Smith-Sgarbossa criteria for acute OMI in patients with LBBB — there are qualitative ST-T wave abnormalities in virtually all leads in Figure-1 (By “qualitative” abnormalities — I mean ST-T wave changes that simply should not be there).
- The dotted RED lines on the ST segment baseline in leads V1-thru-V4 help to highlight the amount of J-point ST elevation (small PINK arrows). As per Dr. Smith — this J-point ST elevation is excessive in lead V2.
- But more than the amount of ST elevation in lead V2 — the ST-T waves in leads V1-thru-V5 are all “fatter”-at-their-peak and much wider-at-their-base than expected, given modest depth of the S waves in these leads (= clearly “disproportionate”). Note the clearly abnormal shape of the straightened ST segment takeoff in leads V1,V3,V4,V5 — with the T wave in lead V2 literally being taller than the S wave is deep. These are all ST-T wave changes that the experienced “eye” instantly knows should simply not be there.
- Lead V6 is remarkable for abnormal ST segment flattening. Viewed in association with the ST elevation and hyperacute changes in the other 5 chest leads — this suggests Precordial “Swirl” in a patient with LBBB (See My Comment at the bottom of the October 15, 2022 post for my synthesis on how to recognize “Swirl” ).
- With regard to the limb leads — Normally with LBBB, the ST-T wave should be oppositely directed (ie, depressed) in left-sided leads with an all-positive R wave The fact that the T wave is upright in both leads I and aVL facilitates recognizing the abnormal ST-T wave response in these leads (RED arrows in I,aVL).
- Finally — there are reciprocal changes in each of the inferior leads (ie, in leads II,III,aVF) — which makes for yet one more sign suggesting acute proximal LAD occlusion.
Bottom Line: To the experienced “eye” in this patient with acute CP — the above findings represent ST-T wave abnormalities in virtually all leads in this tracing. Added to worrisome bradycardia + LBBB + 1st-degree AV block + diffuse low voltage — the “picture” of acute proximal LAD occlusion with ongoing extensive infarction (with urgent need for prompt cath with PCI) — must be assumed until proven otherwise.
- If this conclusion is not quickly reached on seeing this initial tracing — then assistance with the QOH AI ECG Model is urgently needed.
- = = =
- P.S.: With typical LBBB — there should be an all upright R wave in left-sided leads I and V6. Instead we see continued drop-off of QRS voltage from lead V4-to-V5-to-V6, with no more than minimal positivity in this most lateral chest lead (which provides yet one final clue to large-scale loss of myocardium from this patient’s extensive ongoing infarction).
= = =
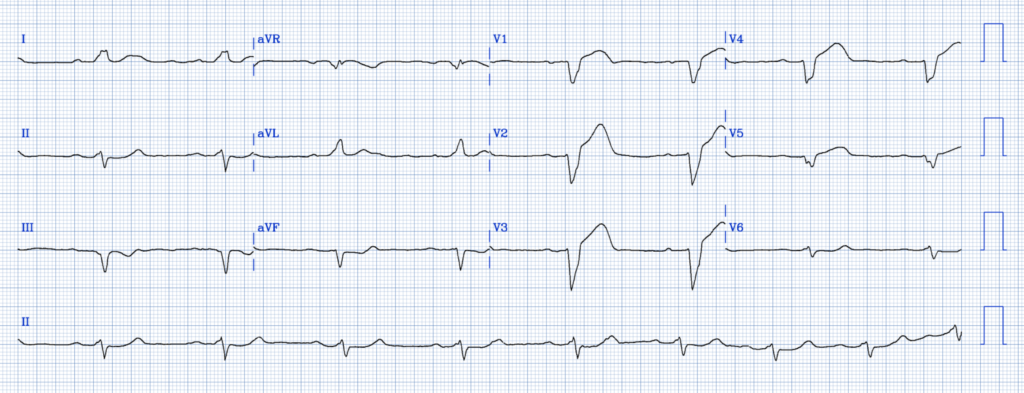
Figure-1: I’ve reproduced and labeled today’s initial ECG (To improve visualization — I’ve digitized the original ECG using PMcardio).
= = =
= = =