I came across this ECG while reading through all the ECGs on the system.
The computer interpretation, confirmed by a cardiologist, is:
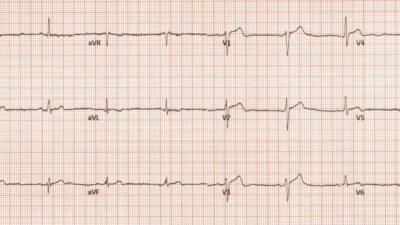
- “Sinus Brady with moderate intraventricular conduction delay, nonspecific T wave abnormality, abnormal EKG”.
= = =
What do you think?
= = =
This is my interpretation: there is subtle STE in III and aVF. In aVF it is “coved” (upwardly convex). The T wave is inverted in III and aVF, and reciprocally upright in aVL (and is very large, a reciprocally upright hyperacute T-wave), with reciprocal STD in aVL. There is ischemic ST depression in V4-V6. This is diagnostic of ACS; it appears to be a reperfused acute inferior OMI.
Later, I sent it to 5 of my “OMI Nerdz” group without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: “reperfused inferior OMI”.
- Although the findings are VERY subtle, they are diagnostic. But they are so subtle that I would only expect a few people in the world to recognize them.
When I saw it, I immediately went to see what happened:
Case presentation:
The patient is a 55-year-old male who presented to the emergency department after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin.
It is unknown when this pain recurred and became constant.
More past history: Hypertension, tobacco use, coronary artery disease with 2-vessel PCI to the right coronary artery and circumflex artery several years prior. Angiogram in a few years back — type III LAD with LAD 60% disease in mid segment. LCX with moderate disease. Mild disease of RCA.
He reported feeling nauseated with emesis. He reported that this chest pain felt different than prior chest pain when he had his STEMI/OMI, but was unable to further describe the chest pain. He denied taking aspirin or antihypertensive medications for the last year and a half. He denied other symptoms, but the remaining history limited given patient emesis.
He was transported from hallway bed to a room with telemetry.
At the time of the above HPI, the patient was sitting on the edge of his bed and ambulatory.
Here is the ECG again:

= = =
Case Continued:
The ECG findings were not recognized.
- The patient had continued chest pain, in spite of the appearance of reperfusion on the ECG; persistent CP with an ischemic ECG is an indication for cath lab activation!
- The patient was placed in waiting room for 10 minutes, then in the hallway because rooms were very hard to obtain. Then he was placed in a room after 30 minutes.
= = =
Arrival at Time = 0
- ECG @ 7 minutes.
- Roomed in hallway @ 17 minutes.
- Moved to room with monitor @ 37 minutes.
- The patient was seen briefly by the physician, who then went to get an ultrasound machine.
- At 47 minutes, when the physician returned, the patient was found to be in ventricular fibrillation with agonal breathing. Resuscitative attempts were initiated quickly.
VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Eventually asystole, and the patient died.
- The first troponin-I (which was drawn prior to arrest, but resulted much later) was 500 ng/L.
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict:
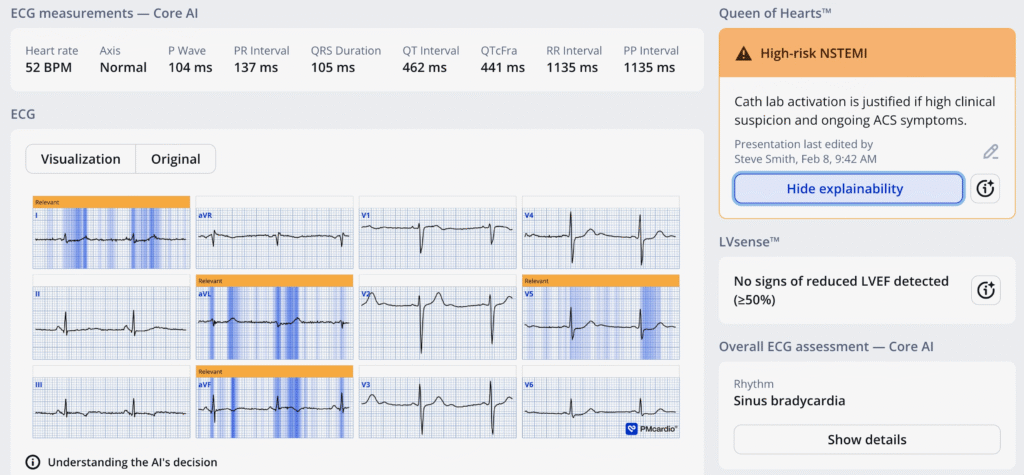
Use the PMCardio Queen of Hearts AI Model and you won’t miss these!!
In the meantime, the lesson here is: Even if you think the ECG is normal or nondiagnostic — in patients with a high pretest probability of OMI, record serial ECGs!!
- Even if the Queen had said “Not OMI with High Confidence,” you should get serial ECGs in a patient who has a high pretest probability.
Does the Queen of Hearts just call everything an OMI? So much so as to be useless? NO! She is very specific. A recent study showed that she could decrease false positive activations from 42% to 8%!! And, at the same time, identify 92% of OMI on the first ECG (vs. 71% for the actual physicians). Specificity was 81% (vs. 29% for physicians).
What if the ECG were indeed truly negtive? This patient’s pretest probability for OMI is extremely high. He has a h/o of 3-vessel disease with stents, and his pain has been on and off for days. These are VERY high risk symptoms. Therefore, no matter the initial ECG, record serial ECGs.
Would it have mattered if the OMI had been diagnosed prior to arrest? Maybe. Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI. Then the patient would have been taken to the critical care area with a defibrillator at his side while waiting for the cath lab to be ready. But as it was, the delay to defibrillation was not long, and it may be that nothing could have saved him. 3-vessel disease can make resuscitation very difficult, since CPR does not perfuse diseased vessels as well as one would like.
= = =
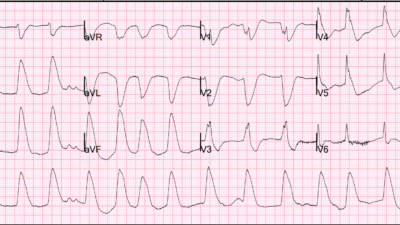
The patient’s baseline ECG from 2 years prior was found later. It was not available initially due to an alternate medical record number:

Here again is the presenting ECG for comparison:

Terrible cases like these can lead to feelings of shame and guilt. We have all had such cases. We have all felt those awful feelings. The past is past, and looking back will only help if we can find things that could have been done differently. And so we share cases like this in the hope that others can learn from them and prevent such deaths.
That is what Emergency Medicine is all about.
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical). As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: Certain AI ECG Modules are CE-marked medical devices under EU MDR and are certified for marketing only in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA.
= = =
======================================
MY Comment, by KEN GRAUER, MD (9/3/2023 — Updated for WordPress on 2/10/2026):
I’ve seen a “common theme” with many of the ECGs that Drs. Smith, Meyers and McLaren present regarding cases they encounter (either personally — or sent to them by other clinicians) — namely:
- HOW can we recognize “that Something“ in an otherwise subtle ECG that immediately tells us, “Beware!” ?
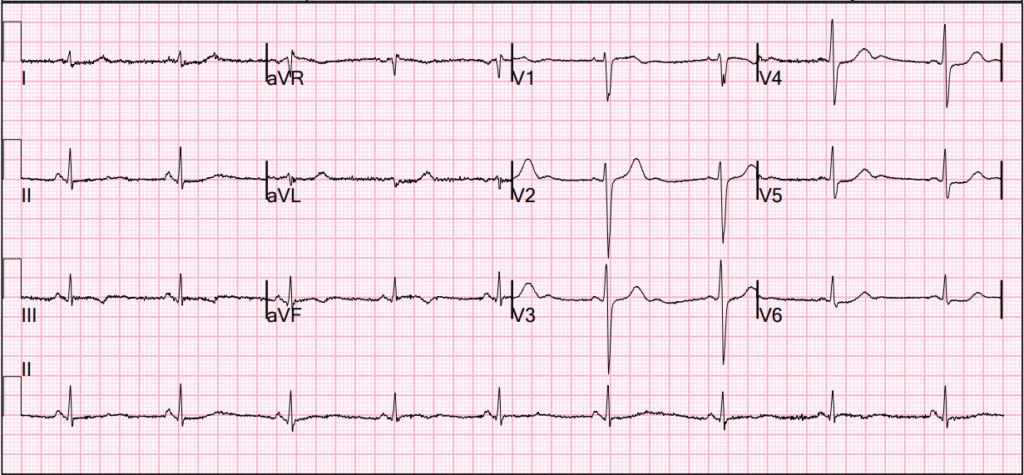
Today’s case provides a perfect example of this clinical challenge. I was shown today’s initial ECG (that I’ve reproduced in Figure-1) — knowing only that this tracing was from a patient in the ED (therefore — a patient presumably with some kind of chest discomfort, albeit of unstated duration and severity).
= = =
Figure-1: I’ve labeled the initial ECG in today’s case.

= = =
MY Thoughts on the ECG in Figure-1:
There is some baseline artifact (particularly in the limb leads) — but the tracing is still interpretable.
- The rhythm in ECG #1 is sinus bradycardia at ~50-55/minute. Intervals (PR, QRS, QTc) are normal. The frontal plane axis is normal at +70 degrees. No chamber enlargement.
With regard to Q–R–S–T Changes:
- There appear to be tiny, narrow Q waves of uncertain significance in the inferior leads.
- R wave progression — is normal, albeit with slightly delayed transition (The R wave becomes taller than the S wave is deep between V4-to-V5) — modest lateral chest lead R wave amplitude — and persistence of S waves through to lead V6.
Regarding ST-T wave abnormalities:
Note in Figure-1 that I’ve labeled abnormal ST-T wave findings (many of which are subtle-but-real) in no less than 10/12 leads!
- To return to the principal point that I raised at the beginning of my comments — that “Something“ that is present in today’s initial ECG that immediately told me “Beware!” — is the shape of the ST-T wave in lead aVL. There simply is No way in a patient with chest pain that this ST segment flattening with disproportionately huge, “bulky” hyperacute T wave in lead aVL was not indicative of recent or acute OMI until proven otherwise.
- To Emphasize: Without this ST-T wave appearance in lead aVL — I’d still recognize the abnormal findings in the other 9 leads. But I’d be less certain about an acute event without more information and prior and/or serial tracings. With the ST-T wave appearance that we see in lead aVL — I knew within seconds that prompt cath was indicated as soon as this could be done.
What are the Other ST-T wave Findings?
- Less marked but similar in appearance — is ST segment flattening with a disproportionately large (hyperacute) T wave in lead I.
- There is subtle-but-real ST coving in the nonelevated ST segments of leads III and aVF — that end with T wave inversion.
- The 3rd inferior lead ( = lead II) — shows definite ST-T wave flattening.
- In the context of the above limb lead findings — I thought the T wave in lead V2 was disproportionately tall, as well as being “fatter”-at-its-peak and wider-at-its-base than expected, given R wave amplitude in this lead.
- ST segments in neighboring leads V3,V4 are clearly straight (flatter) than they should normally be (Normally there is at least slight, upward sloping ST elevation in leads V2 and V3).
- Finally — RED arrows in leads V5,V6 show these flattened ST segments to manifest slight-but-real ST depression.
= = =
Putting It All Together:
In addition to the above noted findings — U waves are seen in leads V3,V4,V5 — so serum K+ and Mg++ need to be checked.
- Given “that Something” in lead aVL, that immediately caught my attention — in association with subtle-but-real ST-T wave abnormalities in 9 additional leads — I felt cardiac cath was indicated as soon as this could be done.
- As noted above by Dr. Smith — recent/acute infero-postero OMI, now with spontaneous reperfusion seemed the most likely explanation — potentially with multi-vessel coronary disease given the lateral chest lead ST depression.
- Once this ECG pattern of recent spontaneous reperfusion is recognized — We are faced with the problem that what spontaneously opens may just as easily (and, at any time) spontaneously reclose — with spontaneous reocclusion of the “culprit” artery presumably being the cause of this patient’s cardiac arrest 47 minutes after arrival. It is for this reason that prompt cath with PCI is still indicated, especially if the patient is still having ongoing CP.
= = =
= = =