Written by Pendell Meyers
A 47-year-old man with known WPW syndrome presented to the ED complaining of left abdominal pain, diarrhea, and chills. He denied palpitations, but is found to have a heart rate of 170 bpm at triage. He states that he occasionally has episodes of tachycardia which usually lasts about 1 hour, which he was instructed to “ride out at home unless they persist.” Other than his heart rate, his other vitals were within normal limits, and the patient did not show any signs of compromised cardiac output or distress.
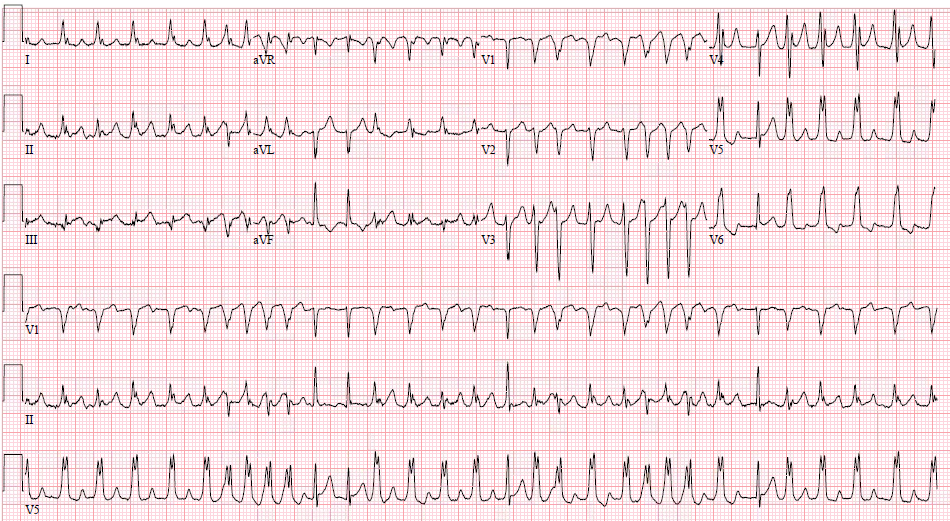
Here is his initial ECG:
 |
| What do you think? |
The ECG shows an irregularly irregular polymorphic tachycardia at approximately 186 bpm. Occasional beats are conducted with narrow, normal morphology, but most are conducted aberrantly with a nonspecific intraventricular conduction delay pattern, which is not actually very wide despite the abnormal conduction. While most of the abnormally conducted beats have the same morphology, the morphology becomes more polymorphic when the rate increases, as seen twice during this ECG, with lead V1 best demonstrating significantly different morphology between QRS complexes. Several beats are conducted at approximately 300 msec after the previous beat, which is extremely unlikely to be the result of a normal AV node conduction.
Because it is irregularly irregular, polymorphic, and has R-R intervals approaching less than 300 msec, the diagnosis is atrial fibrillation with WPW (also called pre-excited atrial fibrillation) until proven otherwise.
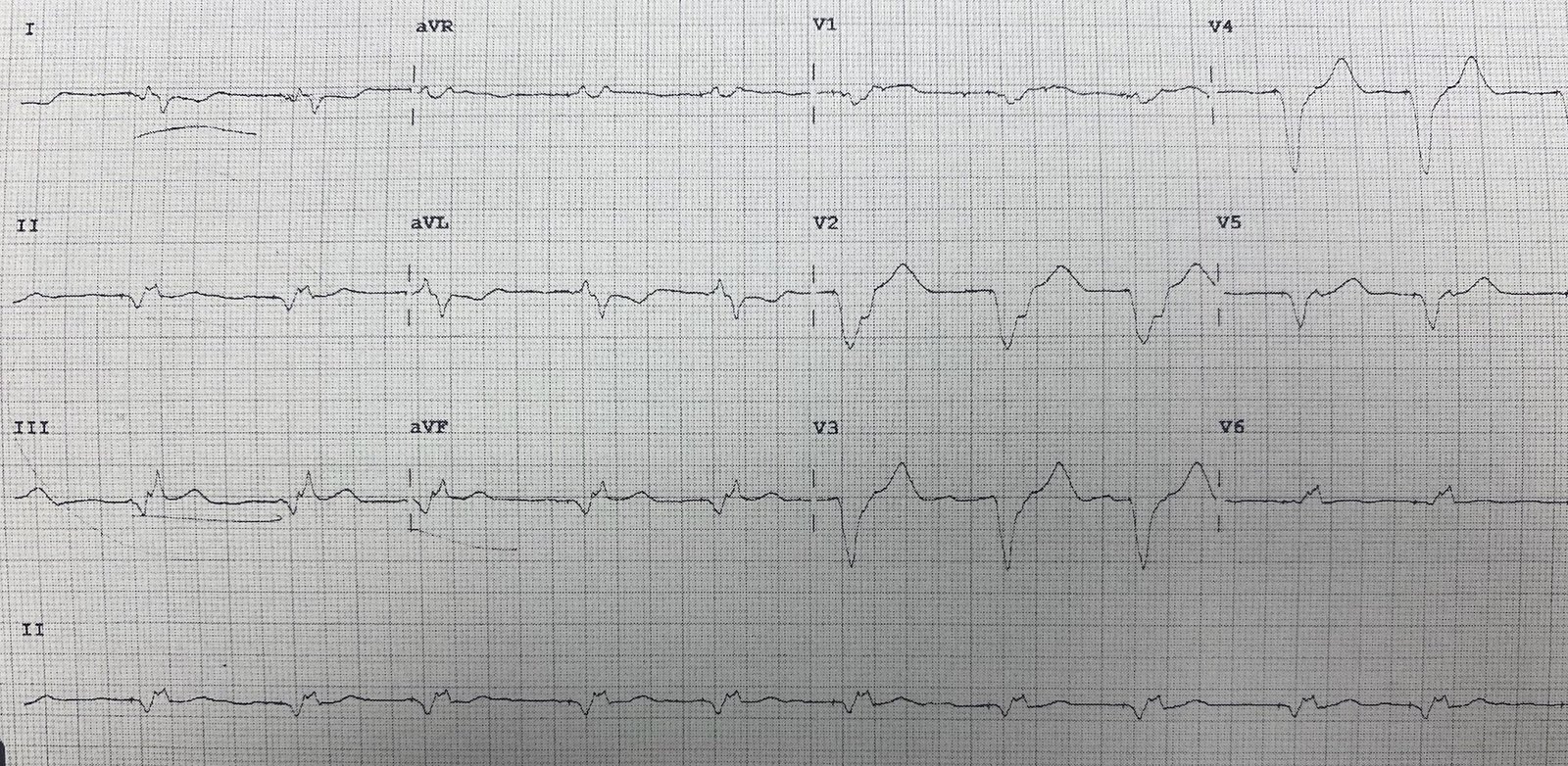
Here is his baseline ECG:
 |
| Sinus rhythm with very short PR interval and subtle delta waves. The QRS morphology matches the most common beats in the presentation ECG above, implying that this is his most common QRS pattern as a result of simultaneous activation via the AV node and accessory pathways. |
Although the patient remained clinically stable and never showed any signs of distress or shock, his heart rate gradually accelerated over the course of the next 30 minutes. He never showed any signs of deterioration, and cardioversion was not attempted. All nodal blockers (BB, CCBs, amiodarone, adenosine) were avoided.
A repeat ECG was performed:
 |
| Extremely rapid rates, approaching 260-280 bpm. It is technically polymorphic (again V1 is most clear), although I must say it is slightly less polymorphic than other examples of AF + WPW that I have seen at rates like this. It is also still irregularly irregular, so it must still be AF. |
We (Smith and Meyers) believe that the best course of action for this persistent dysrhythmia at a rate of nearly 280 bpm, even if the patient is not clinically unstable, is probably just to perform synchronized cardioversion at this time, without waiting for infusions such as ibutilide or procainamide. Dysrhythmias like this which are persistent at such high rates and polymorphic have a high chance of deterioration into VT/VF. We would give etomidate and perform synchronized cardioversion for this. In my practice, it takes a significant amount of time to actually obtain and administer ibutilide or procainamide. If it recurs after cardioversion, of course an infusion will be required.
In this case, however, electrical cardioversion was not performed and the patient did not deteriorate.
Cardiology advised starting ibutilide (a class III antidysrhythmic medication which blocks K channels, increasing the duration of the refractory period, which inhibits conduction and propagation of dysrhythmias). Procainamide (a class Ia Na channel blocker) would also have been reasonable.
Ibutilide was started, followed by conversion to sinus rhythm approximately 20 minutes later.
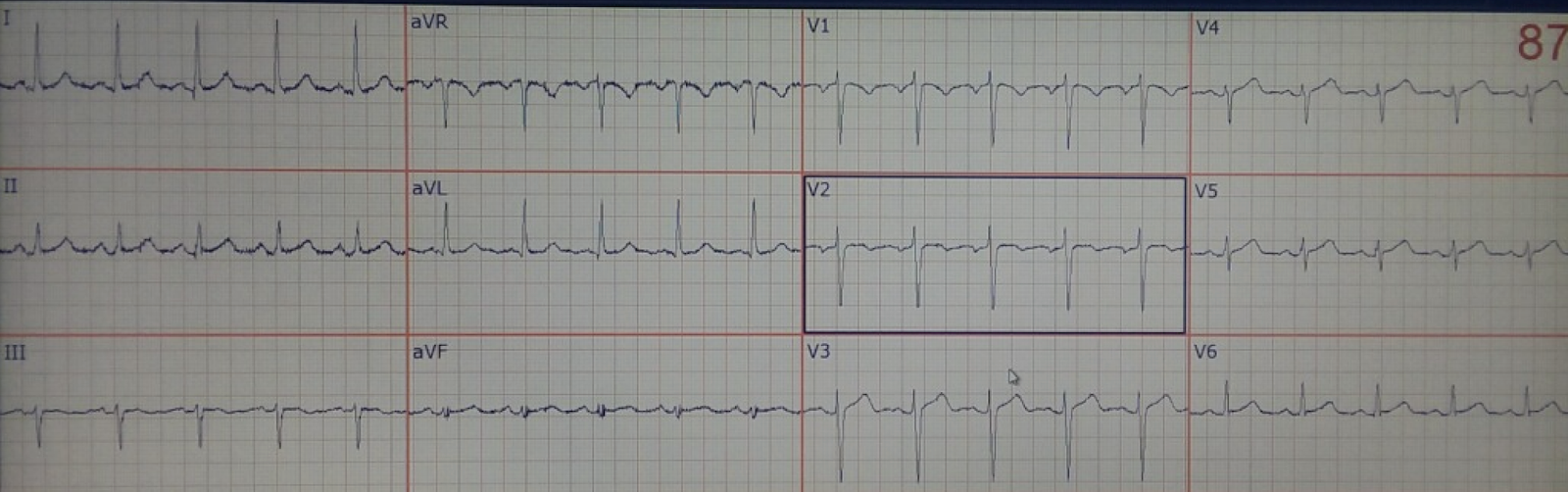
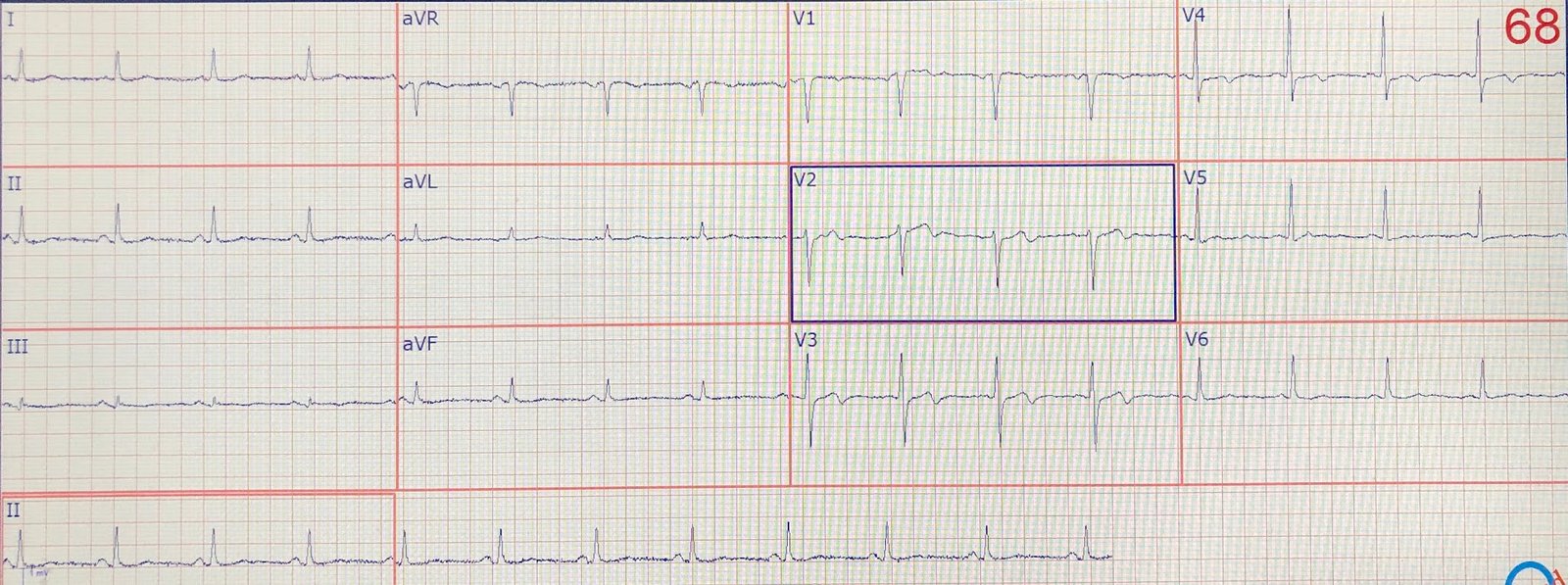
Here is his repeat ECG:
 |
| Sinus rhythm similar to baseline ECG. |
The patient was admitted for observation and treatment of the underlying illness.
Learning Points:
Irregularly irregular polymorphic (usually wide, but not always greater than 120 msec) tachycardia should be assumed to be atrial fibrillation with WPW until proven otherwise.
Adenosine should never be given to any rhythm that is irregular or polymorphic.
Any AV nodal blocker is considered contraindicated in AF with WPW for fear of enhancing conduction through the bypass tract, which theoretically could result in deterioration of the rhythm.
Unstable patients should be cardioverted. For stable patients, procainamide or ibutilide are both accepted pharmacologic agents for this scenario. Synchronized cardioversion with sedation is a reasonable and safe option as well, however it would not be appropriate if the rhythm is intermittently terminating and recurring (because it will simply recur after your cardioversion). Even for seemingly stable patients, the greater the heart rate and more polymorphic the QRS, the more likely the rhythm will deteriorate, and the more appropriate synchronized cardioversion becomes.
Please refer to our tachycardia algorithm (found on our “teaching images” tab: https://drsmithsecgblog.com/p/teaching-images.html), and/or our EMRAP Corependium chapter on Tachydysrhythmias for more information.
See other examples of this rare rhythm here: