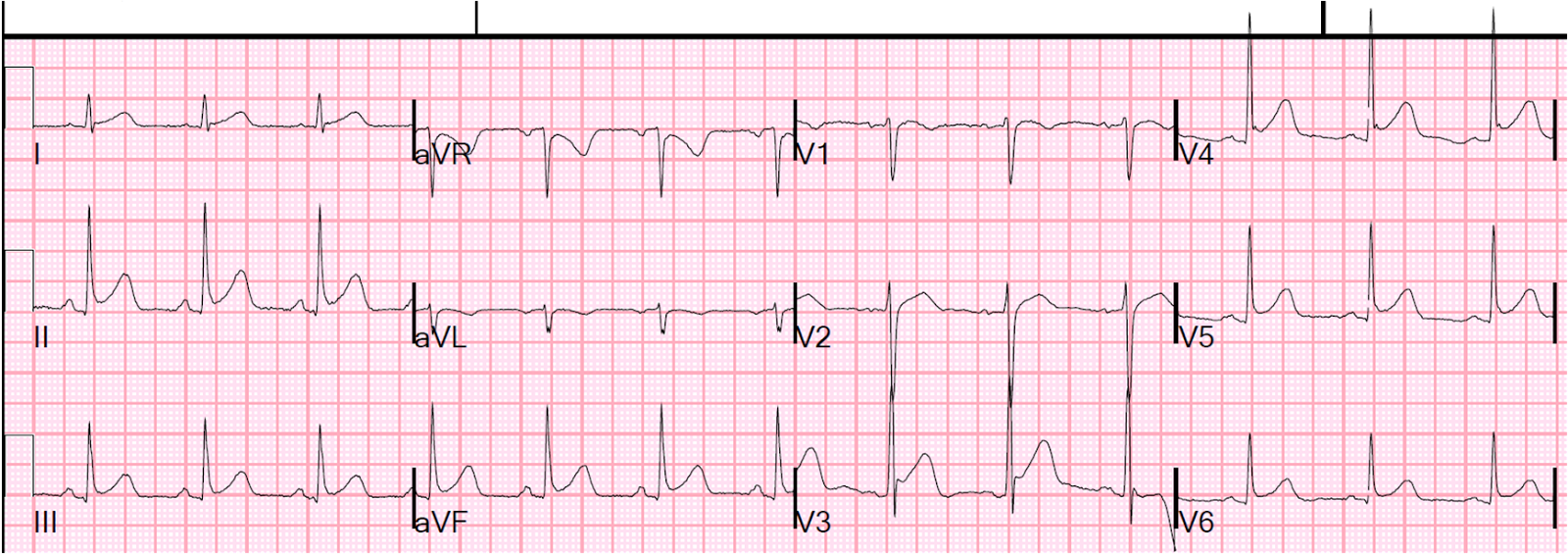
A 40 something presented with chest pain. Here is the ECG:
 |
| QTc 415 ms. What is it? |
The QRS is normal size and duration. So any ST elevation has to by primary, not secondary to LVH, LBBB, etc.
Is it early repolarization? Pericarditis?
There is ST elevation in V1-V3, maximal in V2 at barely more than 1 mm (measured at J-point, relative to PQ junction). The T-wave in V2 is nearly peaked. It does not have the typical wide and fat appearance of an ischemic hyperacute T-wave.
But it has two features that should alert you to LAD occlusion:
1. Look at inferior leads: there is downsloping ST depression with a down-up T-wave in III and aVF. These are highly suspicious for reciprocal changes of LAD occlusion.
2. QRS distortion, which does not happen in early repol or in pericarditis. This is when there is an absence of BOTH and S-wave AND a J-wave in EITHER V2 or V3. This ECG only barely has an S-wave in V3 (the S-wave only goes 0.5 mm below the PQ jct.).
Best Explanation of Terminal QRS Distortion in Diagnosis of Electrocardiographically Subtle LAD Occlusion
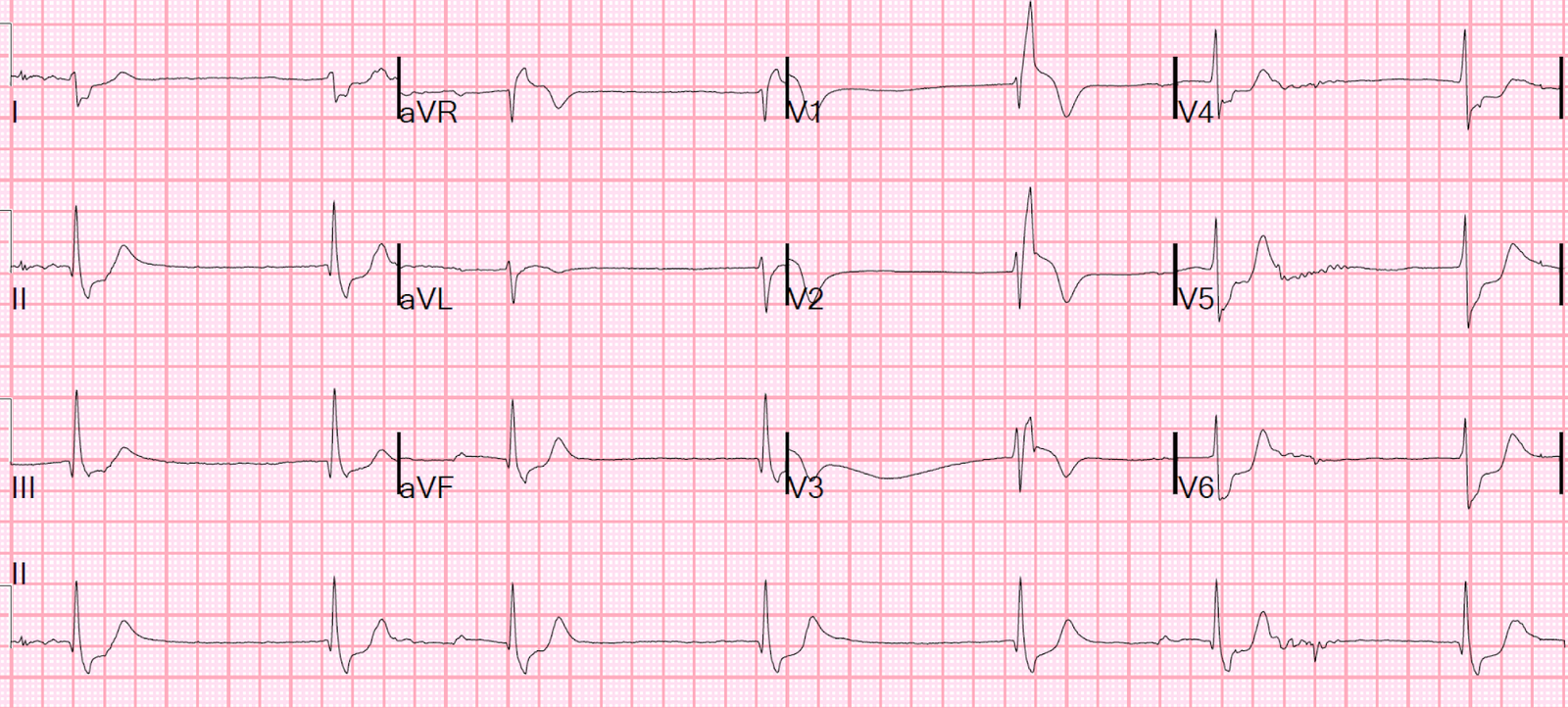
A repeat ECG was done 10 minutes later:
 |
| QTc 419 ms |
Compare V1-V3 side-by-side from the two ECGs:
 |
| There is subtle evolution of the T-waves. They become less peaked, more broad. There is less S-wave in V3 than before. |
The patient was taken to the cath lab and a 100% acute thrombotic LAD occlusion was found. K was normal.