Sent by Pete McKenna M.D. Edits by Meyers and Smith
A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain.
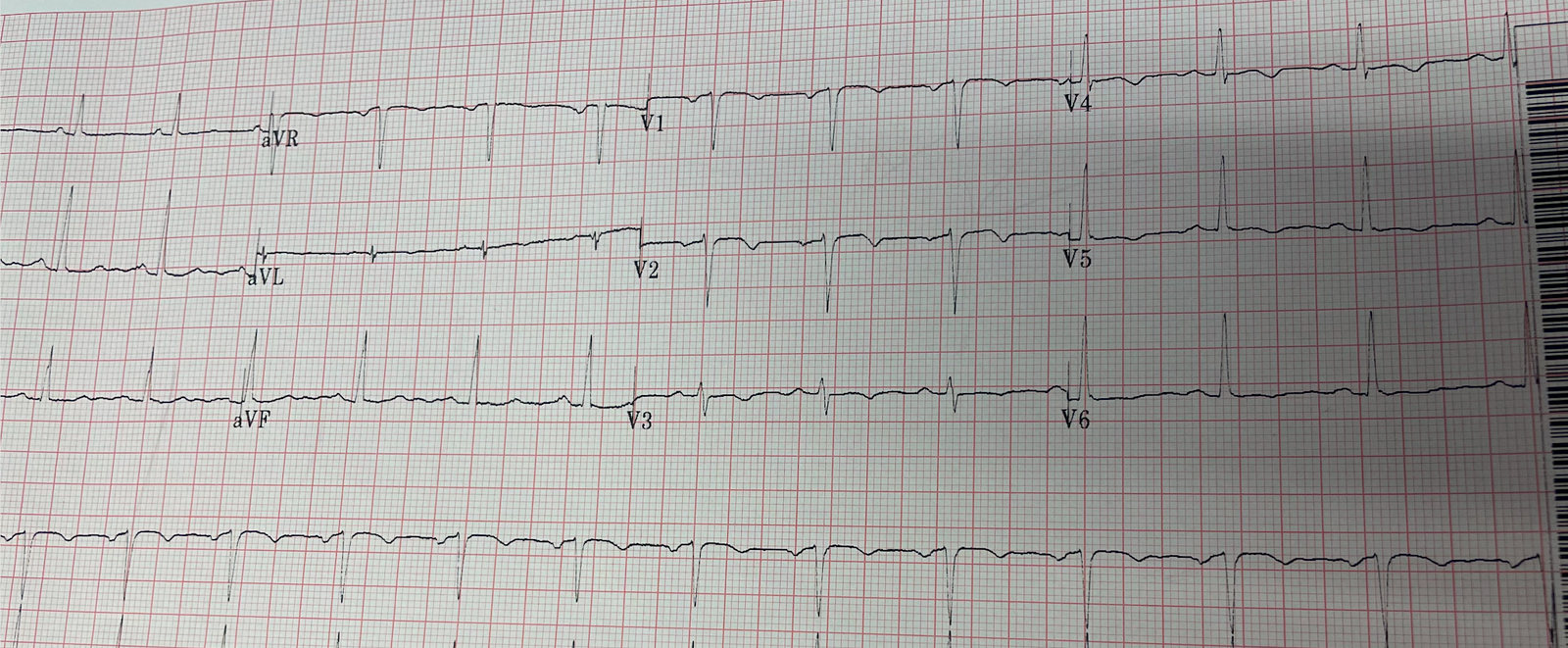
Triage ECG:
 |
| What do you think? |
This is diagnostic of proximal LAD occlusion. This is a huge anterolateral OMI. Deadly. I cannot be anything else.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. There is concordant ST elevation in I, aVL with reciprocal concordant STD in inferior leads, as well as excessively discordant TE in V2-V4.
Queen of Hearts interpretation:

The cardiologist initially was not convinced, stating the ECG was not diagnostic or could not be diagnostic because it was paced. The ED physician attempted to explain the modified Sgarbossa criteria, but without success. (This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm).
===========================================
Modified Sgarbossa Criteria Refresher! Skip if you don’t need this.
===========================================
Here is a visual comparison of the original and modified Sgarbossa Criteria (each has 3 criteria, and only one criterion differs between them: criterion 3 is absolute millimeters in the original, versus proportional in the modified version)

Validation in LBBB:
Meyers HP. Limkakeng AT. Jaffa EJ. Patel A. Theiling BJ. Rezaie SR. Stewart T. Zhuang C. Pera VK. Smith SW. Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. American Heart Journal 170(6):1255-1264; December 2015.
Derivation in LBBB:
–> Smith SW. Dodd KW. Dvorak D. Henry TD. Pearce LA. Diagnosis of Acute Myocardial Infarction in the Presence of Left Bundle Branch Block using the ST Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. Annals of Emergency Medicine 2012; 60(12):766-776.
The ACC likely made this new recommendation for the MSC in ventricular paced rhythm in large part due to the “PERFECT” Study (Meyers is an author, and Smith was the senior author):
In which we compared ventricular paced OMIs with Non-OMIs and MI-ruled out patients. The modified Sgarbossa criteria were more sensitive than the original Sgarbossa criteria (81% vs. 56%) with maintained high specificity.
===========================================
Back to the case:
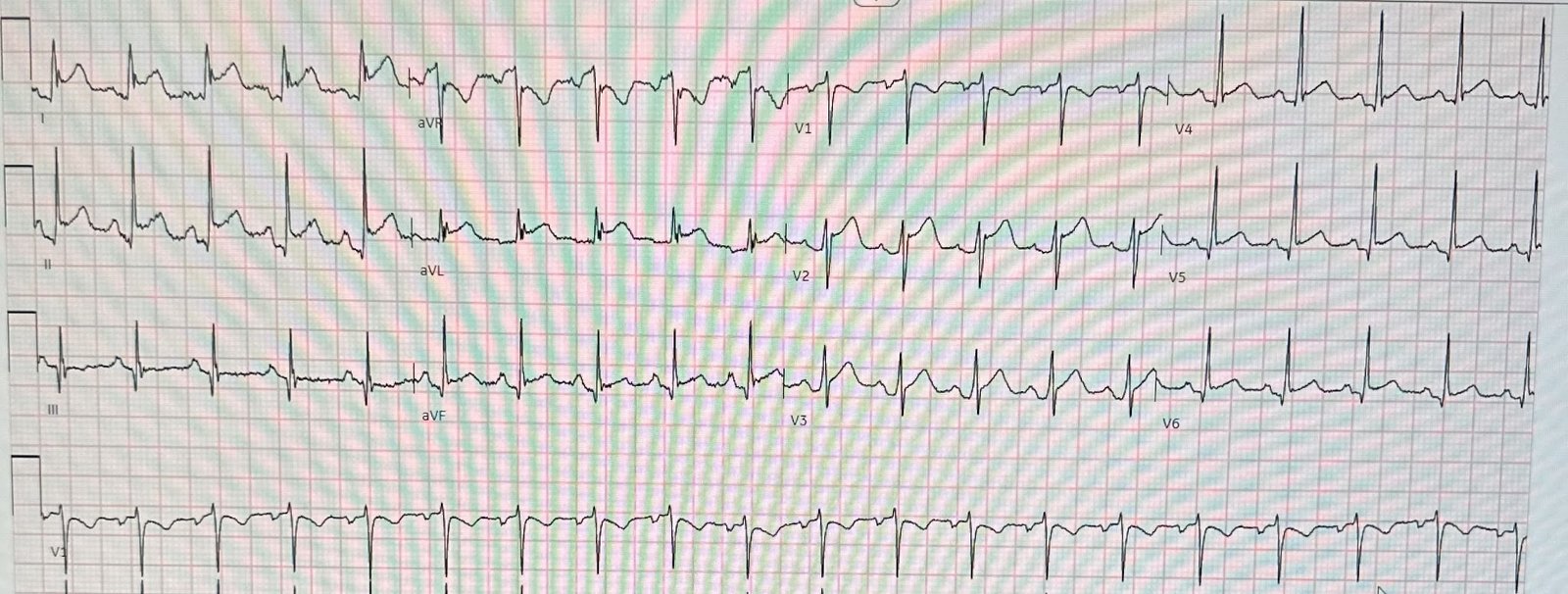
So next the ED physician simply collected serial ECGs. At 20 minutes from initial ECG, the patient’s native rhythm spontaneously usurped the rhythm from the pacemaker:
 |
| No knowledge or guidelines needed to see the OMI findings now! LAFB, atrial flutter, anterolateral STEMI(+) OMI. South African flag pattern, plus precordial swirl pattern. |
Queen of Hearts interpretation:

Now the cardiologist considered it “STEMI”! So the patient was taken for emergent cath, showing:
Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
Impella (cardiac output augmentation device) placed for cardiogenic shock
Unfortunately, the patient progressed to multiorgan failure with worsening cardiac output despite being maxed on pressors and a balloon pump. He expired 4 days later.
Interestingly, this patient was seen in the ED for hypertension and headache 3 days earlier. No labs were performed. EKG and CT head were performed. Imaging was negative and he was discharged home. EKG shown here:
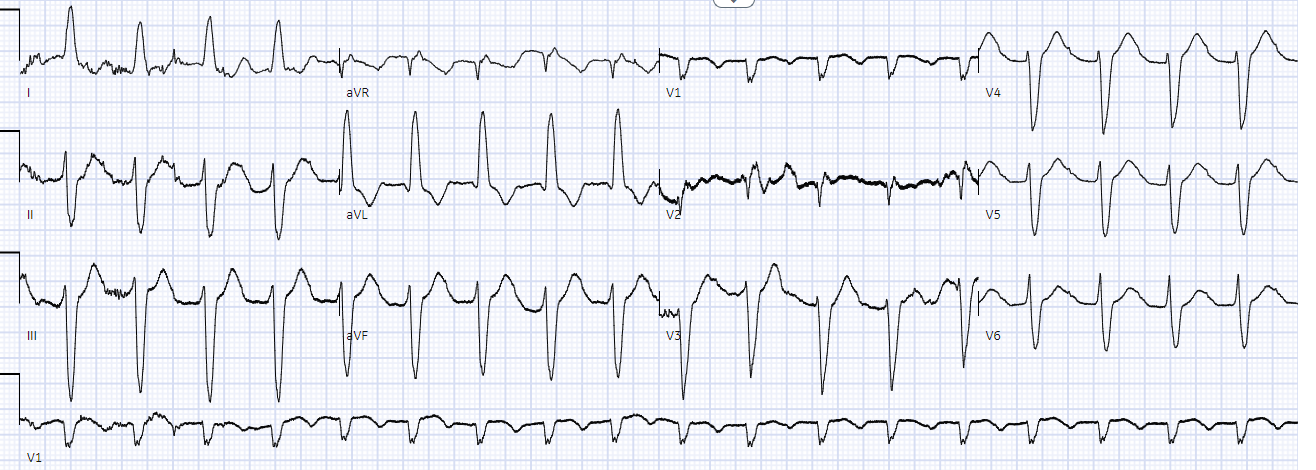 |
| LAFB with no clear signs of OMI or ischemia. |
Queen of Hearts Interpretation:

Would 20 minutes earlier diagnosis have made a difference in his clinical outcome? Maybe not in this case, but we must strive to find this diagnosis in all patients as rapidly as possible.
Learning Points:
Now, even according to the ACC, you should know modified Sgarbossa criteria for both LBBB and ventricular paced rhythm and consider it diagnostic for OMI, and a “STEMI equivalent”, in the appropriate clinical context.
Sometimes repeat ECGs make the difference.
AI will soon be available that can do this.
Why is there this notion that myocardial infarction cannot be diagnosed in the setting of ventricular paced rhythm? Here Dr. Smith pastes the intro to the PERFECT Study:
Electrocardiographic Diagnosis of Acute Coronary Occlusion Myocardial Infarction in Ventricular Paced Rhythm Using the Modified Sgarbossa Criteria
Introduction
Patients with ventricular paced rhythm and symptoms consistent with acute coronary syndrome (ACS) pose a diagnostic challenge due to a long-held misperception that myocardial infarction cannot be diagnosed from the 12-lead electrocardiogram (ECG) in the setting of ventricular paced rhythm.1,2 This decades-old belief, previously also held for left bundle branch block, was based on the fact that both ventricular paced rhythm and left bundle branch block cause secondary repolarization abnormalities and may obscure Q-waves on the ECG.3,4 Q-waves defined the diagnosis of myocardial infarction before modern cardiac imaging was widely available. However, Q-waves diagnose old myocardial infarction, and the notion that myocardial infarction cannot be diagnosed in patients with ventricular paced rhythm or left bundle branch block was inaccurately extended to include the diagnosis of acute myocardial infarction. Immediate ECG diagnosis of an acute coronary lesion resulting in occlusion myocardial infarction is critical in the modern reperfusion era.5 It would be a significant advancement if such a diagnosis could be rapidly made with the ECG.5, 6, 7 Despite this, standardized criteria for diagnosing occlusion myocardial infarction in the presence of ventricular paced rhythm have not been established. Patients with ventricular paced rhythm and occlusion myocardial infarction are, therefore, less likely to receive emergency reperfusion therapy, and they have higher adjusted mortality rates than patients with native cardiac conduction.8,9 Furthermore, patients with ventricular paced rhythm who undergo rapid reperfusion therapy have a lower adjusted mortality rate than those who do not.8,9
The most recent American College of Cardiology and American Heart Association ST-elevation myocardial infarction (STEMI) guidelines (2013) give no direction on diagnosing occlusion myocardial infarction in patients with ventricular paced rhythm.10 In 2018, the European Society of Cardiology guidelines11 and the fourth universal definition of myocardial infarction12 suggested utilizing the original Sgarbossa criteria (Figures 1A to 1C) for diagnosis of occlusion myocardial infarction in both left bundle branch block13,14 and ventricular paced rhythm.15, 16, 17 Those guidelines cite ECG similarities between the 2 conditions but fail to highlight the low sensitivity of the original Sgarbossa criteria. There are 2 primary reasons for this low sensitivity.18,19 First, the derivation of the original Sgarbossa criteria utilized a biomarker (creatinine kinase-MB) definition of AMI, resulting in a case group of patients with both occlusion myocardial infarction and nonocclusion myocardial infarction. Second, the 5-mm discordant ST-elevation criterion of the original Sgarbossa criteria is absolute and not based upon the electrocardiographic principle of proportionality. Smith et al18 derived the modified Sgarbossa criteria (MSC) (Figures 1D to 1F) utilizing angiographic outcomes and defining excessively discordant ST-elevation relative to the amplitude of the preceding S-wave. In both the derivation and validation studies of the MSC, sensitivity was significantly higher than that of the original Sgarbossa criteria (91% versus 52% and 80% versus 49%, respectively; P<.001 for all) and high specificity was maintained (90% versus 98% and 99% versus 100%, respectively; P=NS for all).20
The primary objective of the Paced Electrocardiogram Requiring Fast Emergent Coronary Therapy (PERFECT) study was to compare the sensitivity and specificity of the MSC with those of the original Sgarbossa criteria for the diagnosis of occlusion myocardial infarction in patients with ventricular paced rhythm. We hypothesized that the MSC would be more sensitive than the original Sgarbossa criteria while maintaining high specificity.
![]()
===================================
MY Comment, by KEN GRAUER, MD (5/8/2023):
===================================
I remember the days in the mid 1980s when the automatic dictum was — “You can not diagnose acute myocardial infarction when there is either LBBB or a paced rhythm”. And I remember Dr. Barney Marriott saying, “Not so fast; Sometimes you can!” — and Dr. Marriott showed us how, by simple qualitative assessment of the ECG to see IF there were ECG findings that just shouldn’t be there.
- Some 10 years later — Sgarbossa published criteria for recognition of acute STEMI despite LBBB — with these criteria now vastly improved by Dr. Smith modifications that account for relative size of ST-T wave deflections depending on QRS amplitude in that lead being looked at.
- The above said — it’s hard to believe we are nearly 40 years after Dr. Marriott was already teaching qualitative assessment — and certain clinicians remain “stuck” in the old “automatic dictum”.
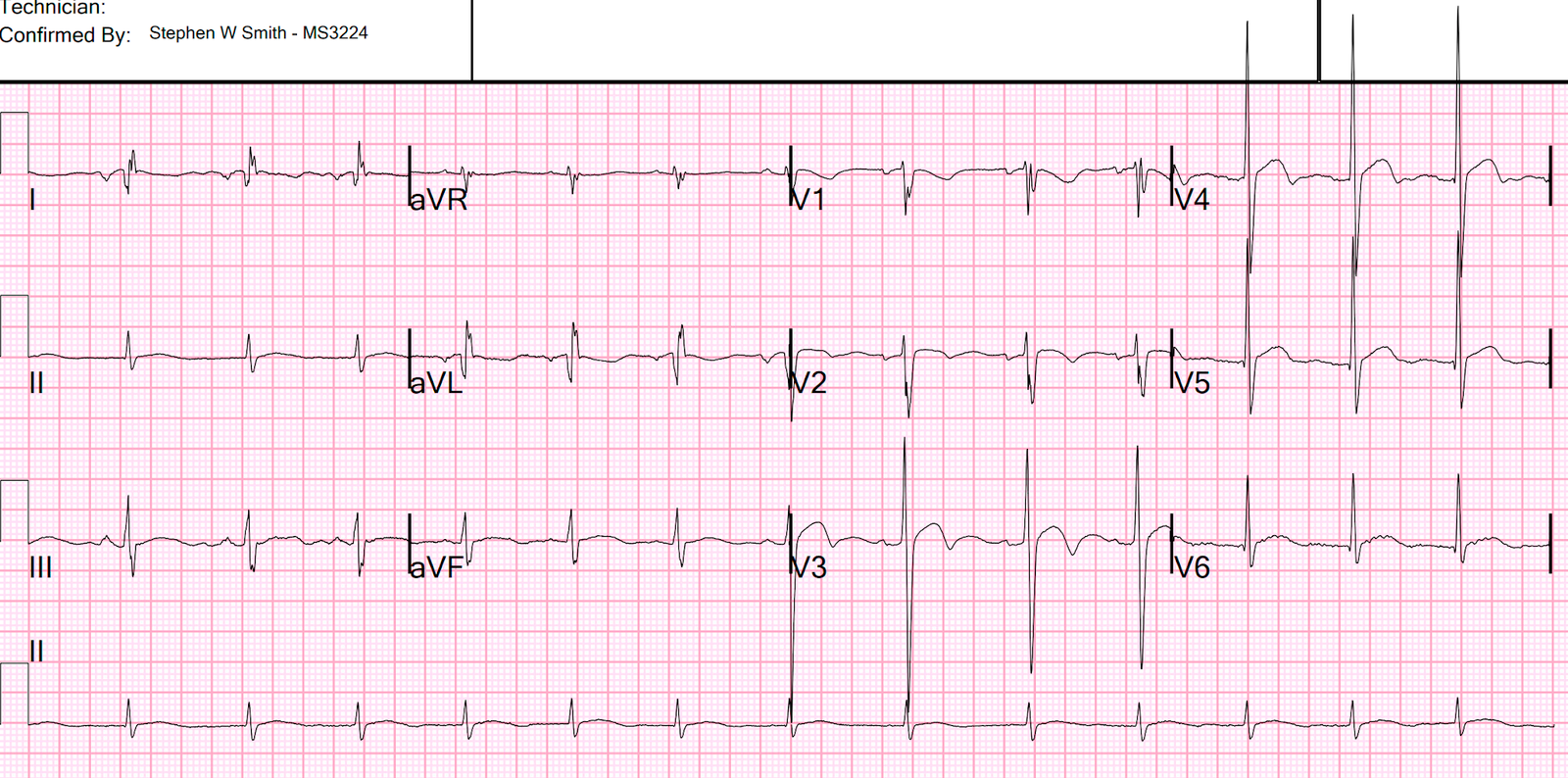
Smith-Modified Sgarboosa Critera have made a tremendous impact in advancing rapid recognition of acute occlusion infarction in LBBB and pacemaker tracings. That said — simple qualitative assessment of the initial Triage ECG in today’s case (that I have reproduced in Figure-1) — is all that should be needed to instantly recognize the extensive ongoing STEMI in this pacemaker tracing.
- It is true that assessment of pacemaker tracings for acute ST-T wave changes can be challenging. Sometimes subtle ST-T wave deviations that would have been recognized had there not been pacing may be hidden within the secondary ST-T wave response to the pacemaker. But there should be no mistaking in today’s initial tracing that there are ST-T wave abnormalities that just should not be there!
- Fragmentation and artifact (and possibly already in the inferior leads, the Atrial Flutter pointed out by Dr. Meyers that became obvious in the repeat ECG) combine to make assessment of ST-T wave changes on many of the leads in ECG #1 difficult.
- That said — the ST segment baseline is clear in leads I and aVL (RED dotted lines) — and there can be no doubt that the coved, 3-4 mm ST elevation in these leads just should not be there.
- Assessment of lead III is a bit more challenging — but in the context of clear abnormality in leads I and aVL — there should be no doubt that there is equally marked reciprocal ST depression in lead III (BLUE line in this lead).
- It is fortunate that the ED physician in today’s case knew to continue obtaining ECG that eventually convinced the consulting cardiologist — but that should not have been needed.
 |
| Figure-1: The initial ECG in today’s case. (To improve visualization — I’ve digitized the original ECG using PMcardio). |