Written by Pendell Meyers
A teenager was playing basketball when he suddenly developed palpitations and lightheadedness. He presented soon afterward at the Emergency Department with ongoing symptoms.
Mentation and blood pressure were normal. He had no chest pain or shortness of breath. Heart rates on the monitor fluctuated from 180-250 bpm.
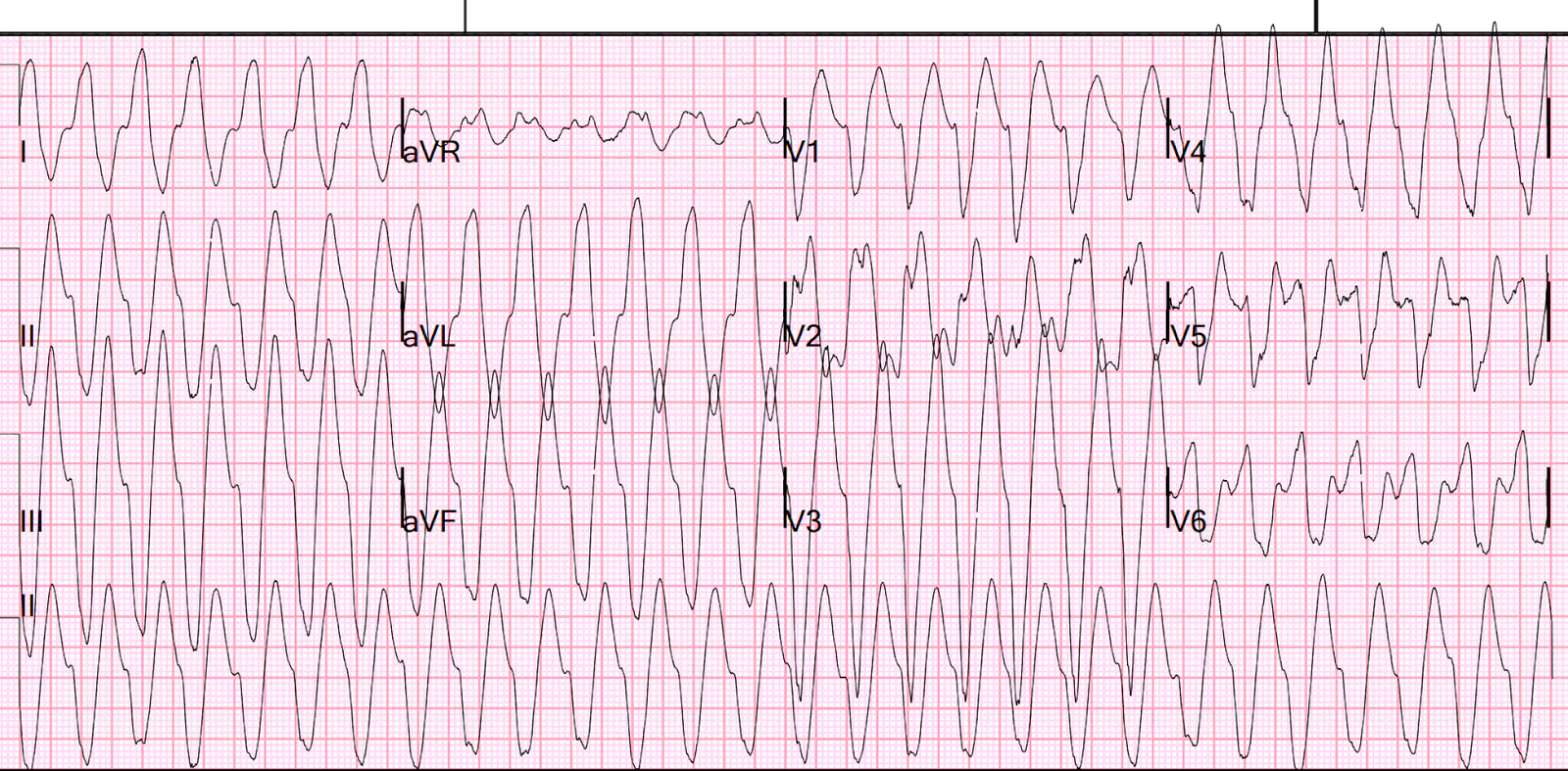
Here is his triage ECG:
 |
| What do you think? |
The ECG shows an irregularly irregular polymorphic wide complex rhythm, with some R-R intervals as short as approximately 220 msec or even less. But it is not disorganized enough to be polymorphic ventricular tachycardia. The rhythm is therefore atrial fibrillation with WPW until proven otherwise.
What do you want to do?
Smith: I always cardiovert. It is far less toxic than any medication. And quicker. You only need to know how to do procedural sedation.
1gm procainamide was given over 20 minutes without successful change in rhythm.
Sedation and cardioversion was then performed:

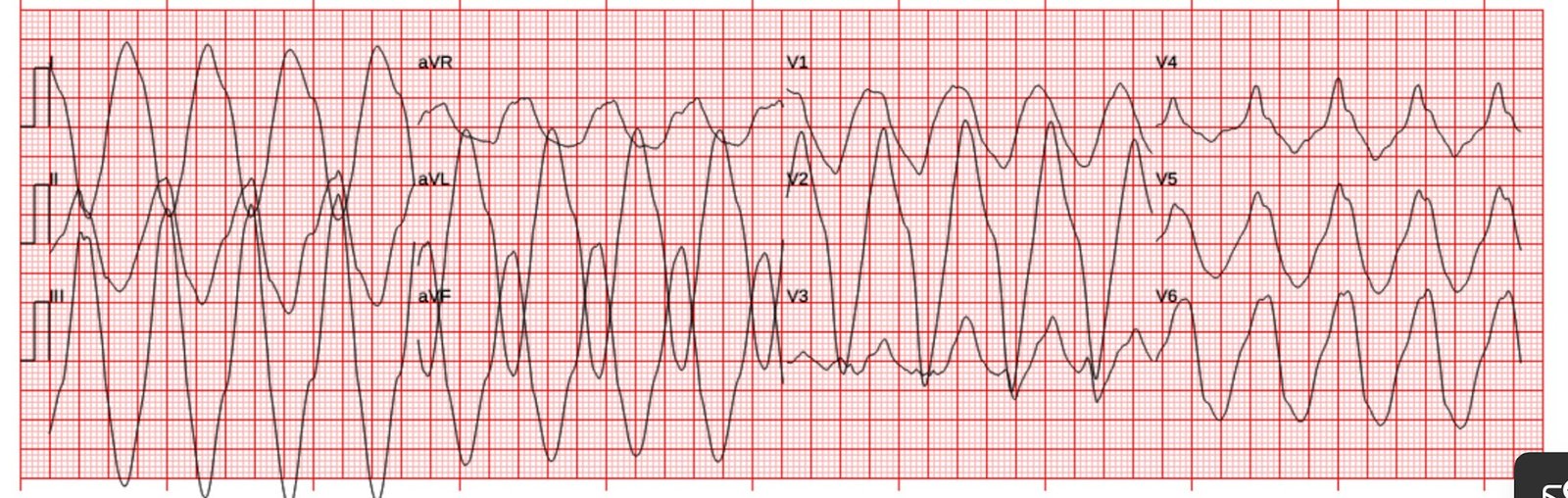
Here is the repeat ECG after conversion:
 |
| Sinus rhythm with delta waves. |
The patient did well and was referred for ablation.
Learning Points:
Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy.
AF with WPW can sometimes be differentiated from AF with aberrancy because AF with WPW may show polymorphic QRS complexes and very short R-R intervals (200 msec or less, but any R-R interval less than 240 ms — 6 little boxes — is likely to be AF with WPW).
WPW can simulate particular aberrancies such as LBBB, and confuse the reader into missing the diagnosis of WPW.
The way to differentiate Atrial fib with LBBB or other aberrancy from Atrial fib WPW is to look for polymorphic QRS complexes, as are clearly seen in the first ECG, and to look for the very short R-R intervals.
See our other cases of AF with WPW: