A 40-something man presented with with 10/10 chest pain after cocaine use. The chest pain had been present for 1 hour.
On arrival in the ED, a Bedside echo showed good function.
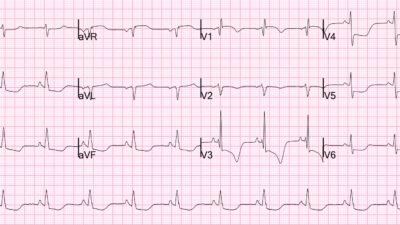
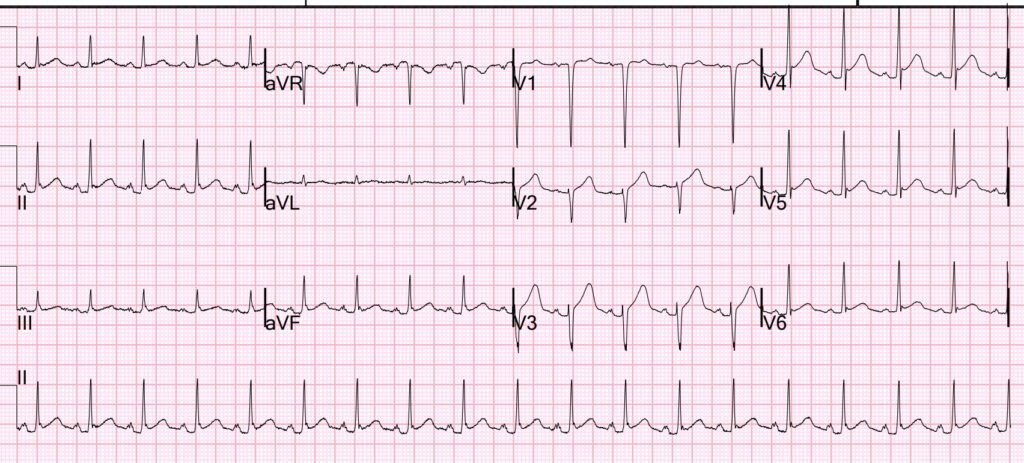
Here was the initial ECG:
What do you think?
I was shown this ECG with clinical context and I interpreted the ECG as Normal variant ST Elevation.
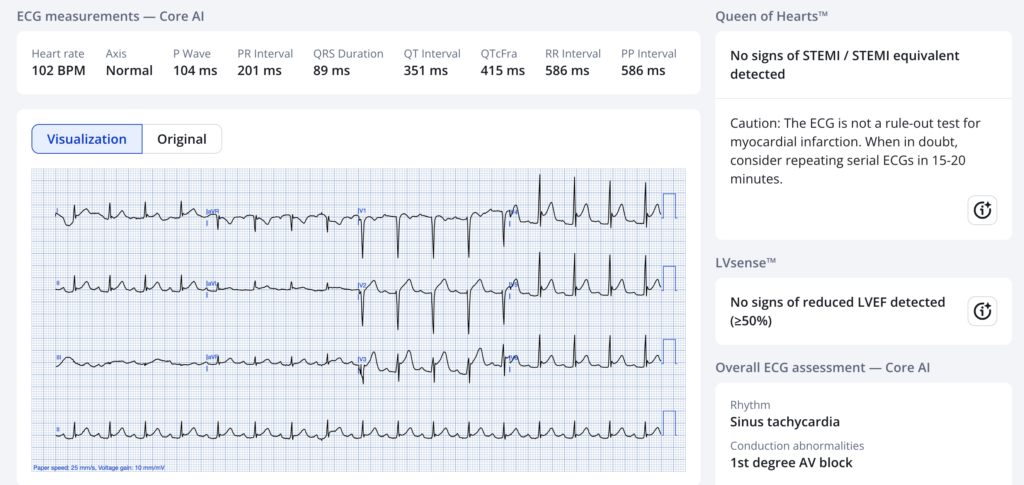
The PMCardio Queen of Hearts agrees:
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical). As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: Certain AI ECG Modules are CE-marked medical devices under EU MDR and are certified for marketing only in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA.
Critical: Chart review shows that he had a CT coronary angiogram 3 months prior that showed completely normal coronary arteries
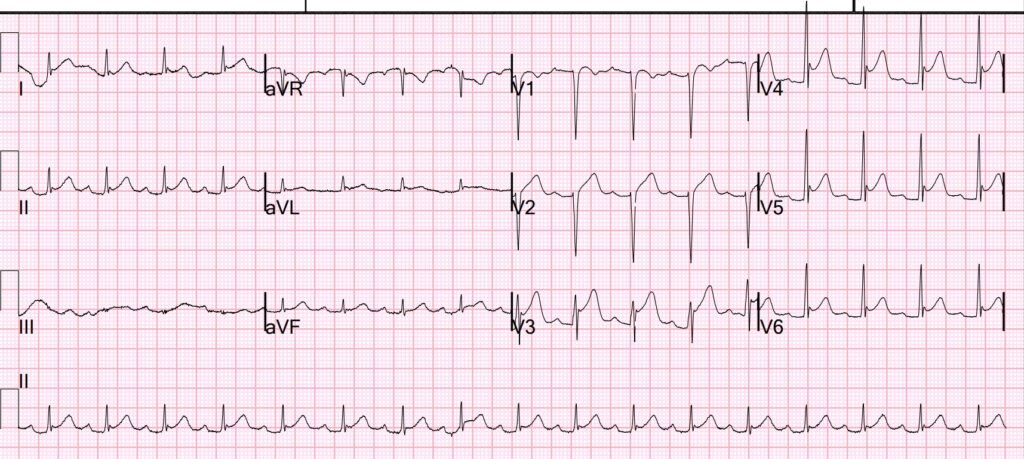
Then we looked for an old ECG for comparison:
There is ST Elevation here as well, though not as marked.
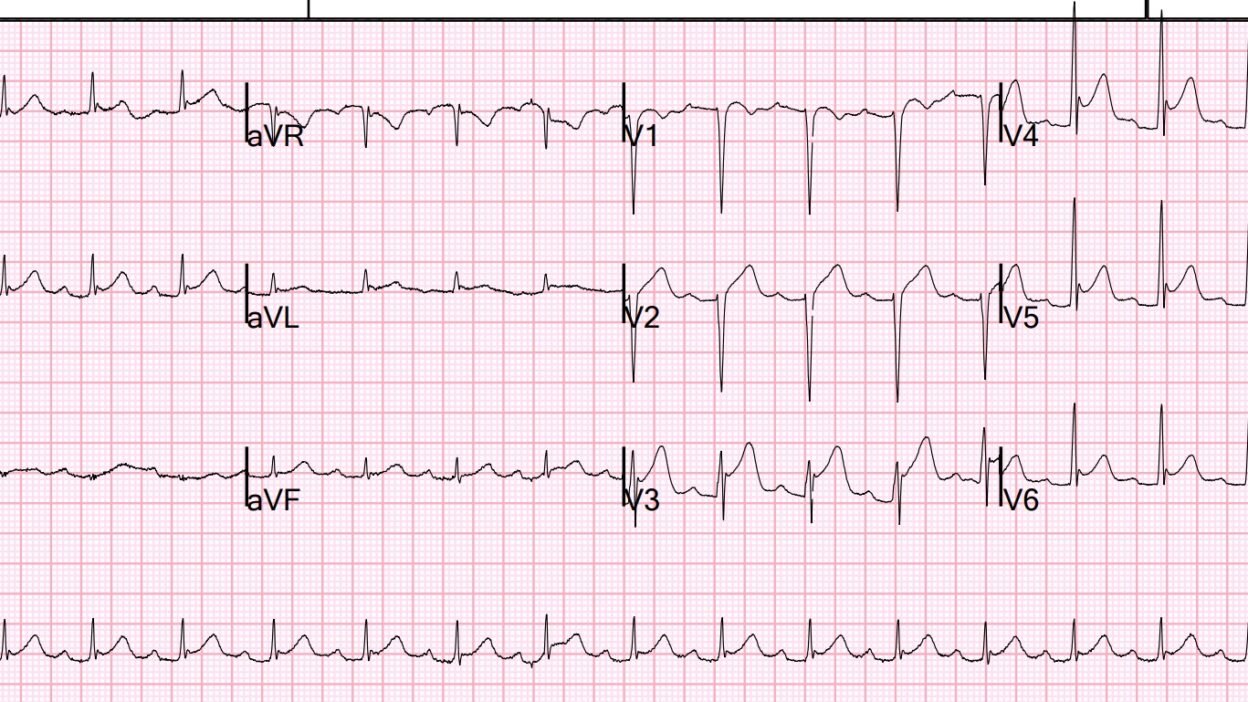
Later, I saw that the patient had arrived by ambulance, so I looked for the prehospital ECG and found it:
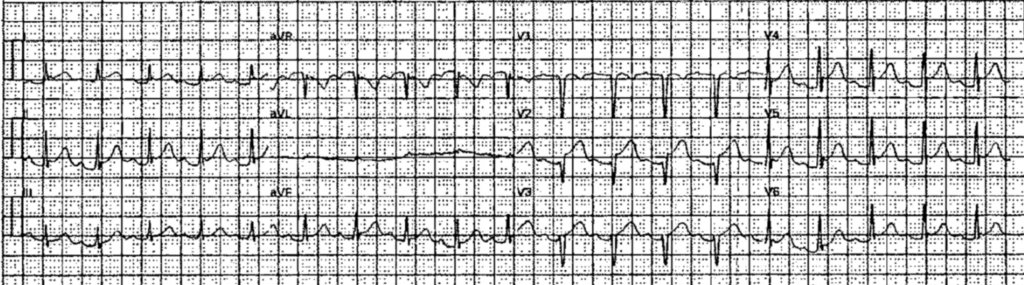
Smith: this is much more worrisome than the initial ECG above. V2 appears to have a hyperacute T-wave. If I saw this without the history of a normal CT coronary angiogram, I would activate the cath lab. This shows how critical a bit of chart review can be.
What does the Queen think of this?

Raw output was 0.36. A result from 0.30 to 0.50 is indeterminate. An indeterminate result has a quite high specificity, so you should be worried when you get this result.
Cardiology was consulted
A formal bubble contrast echocardiogram showed no wall motion abnormality:
–Normal left ventricular cavity size, normal wall thickness and normal LV
systolic function with estimated left ventricular ejection fraction of 55%.
–There is no left ventricular wall motion abnormality identified.
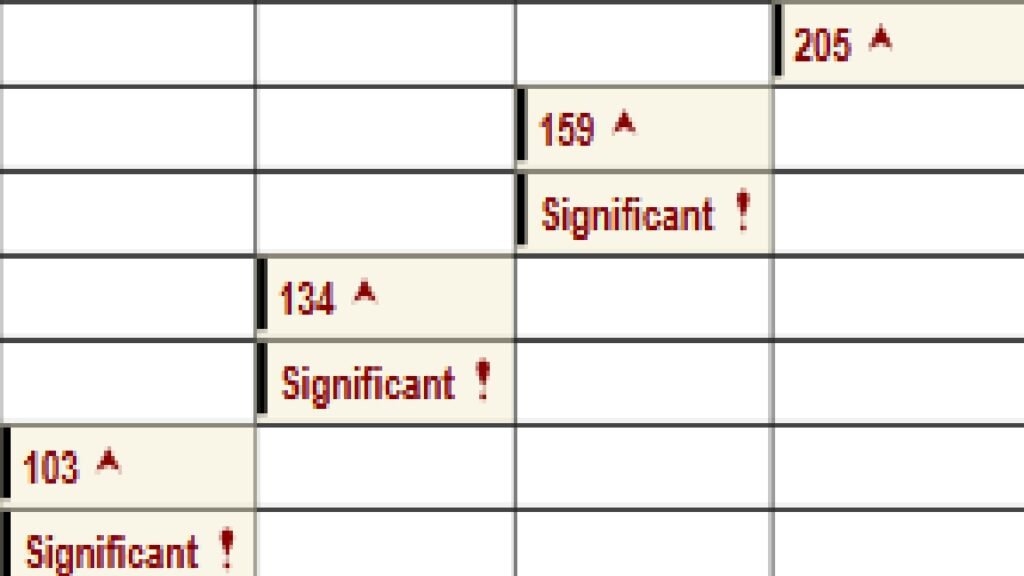
Troponin I were slightly elevated and decreasing over hours:
This is a paraphrased assessment from Cardiology, which I agree with:
Patient presented with non radiating substernal chest pain 10/10. Chest tightness, that is worse with palpation. Prior to admission had used both cocaine and marijuana. States pain not associated with use. Nothing has made it better or worse. Does not notice a change sitting up or increased pain when breathing in. Symptoms have been ongoing for the last few months. Pain not relieved with nitro. Previous workup with TTE, CT coronary angiogram was normal on recent visit. EKG with diffuse ST elevations, and PR depressions.
Very low suspicion for ACS given these findings and presentation. Troponin elevation is thought to be secondary to demand ischemia. Chest pain has been largely unchanged and constant over the last few months. Trops down trending from 205 to 130s. Elevated trops most likely secondary to supply demand mismatch (lactate improved from 4.3 -> 1 following fluids), however pericarditis vs myocarditis cannot be excluded. Chest pain could be due vasospasm from substance use, SK/costochondritis component. No need for angiogram.
Smith: I think the ECG represents normal variant ST Elevation. Subsequent ECGs did not evolve, proving that this is normal variant (both ischemia and pericarditis should evolve).
= = =
======================================
MY Comment, by KEN GRAUER, MD (3/21/2026):
The distinction between ST elevation from a repolarization variant vs acute infarction can be difficult. And when the patient just ingested cocaine — this distinction becomes much more difficult.
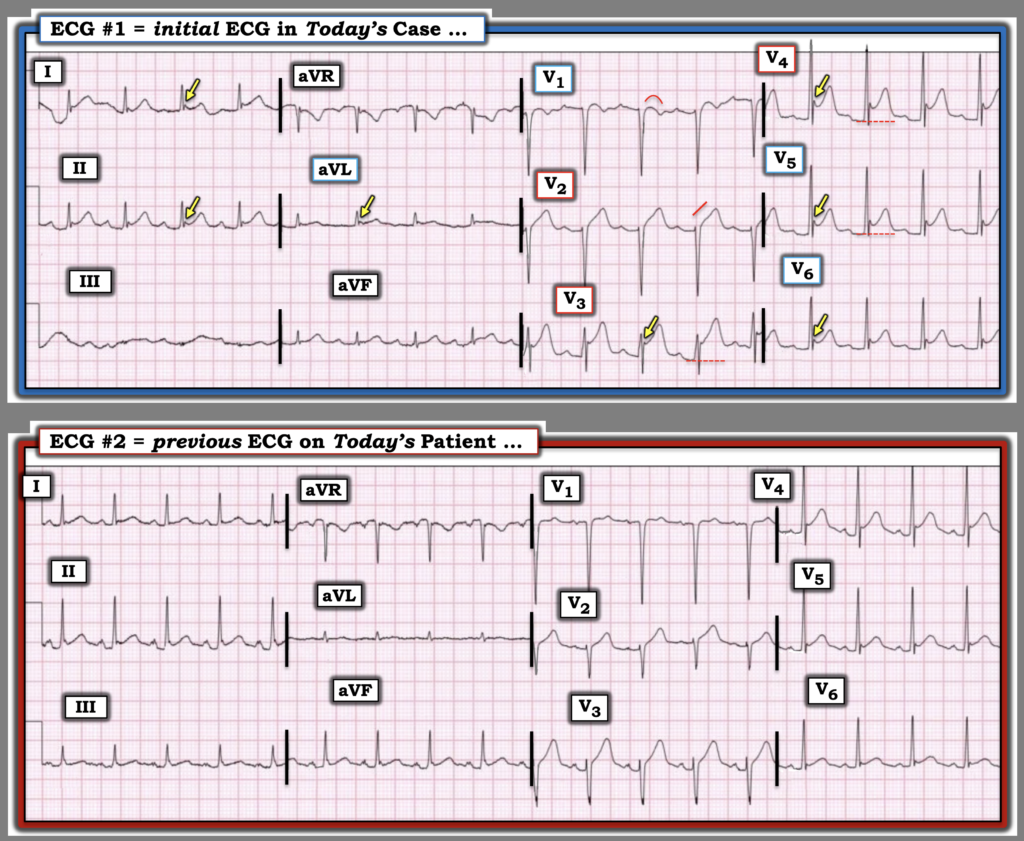
- I focus My Comment on the first 2 ECGs in today’s case — which for clarity, I’ve reproduced in Figure-1.
= = =
The Initial ECG in Today’s CASE:
The sequence in which I reviewed today’s case — was to first only see ECG #1, told only that this patient presented to the ED (Emergency Department) with new CP (Chest Pain) after cocaine use. My thoughts on the initial ECG in Figure-1 were the following:
- The rhythm is sinus tachycardia (at a rate just over 100/minute).
- Intervals (PR,QRS,QTc) and the frontal plane axis are normal. Voltage looks generous (deep anterior S waves) — but falls shy of criteria for LVH in this 40-something man.
- Multiple leads show ST elevation (ie, leads I,II,aVL; and V2-thru-V6) — albeit with an upward-concavity morphology (“smiley” configuration) that is so commonly seen with repolarization variants.
- In support of a repolarization variant is the absence of Q waves — the lack of reciprocal ST depression — and the presence of J-point notching in leads with ST elevation (YELLOW arrows).
- The above said — of potential concern was: i) The amount of ST elevation in selected leads is dramatic (= 5 mm in lead V3; nearly 4 mm in lead V4); — and, ii) Although 7/8 leads showing ST elevation manifest a benign-appearing upward concavity — there is definite ST segment straightening in lead V2, and a somewhat unusual ST segment coved shape in lead V1.
- MY Impression: Overall — I thought ECG #1 looked most like a benign repolarization variant, though the reservations I state in the above bullet left me less than 100% certain of this.
= = =
Once the Previous ECG was Found …
I next saw the previous ECG that is shown in Figure-1.
- Of note — We are not told the circumstances under which ECG #2 was recorded. And, the fact that we again see sinus tachycardia (at a slightly faster rate ~110/minute) suggests that this previous ECG may have also been recorded during an ED visit for cocaine use.
- Once again — voltage is generous (the S wave = 20 mm in lead V1 consistent with voltage criteria for LVH) — and once again, there is upward-concavity ST elevation in multiple leads.
- The above said — my potential concern regarding ECG #1 was increased on now seeing this prevous ECG because: i) The amount of ST elevation is significantly less in all of the chest leads in this previous ECG, than it is in ECG #1; — and, ii) Both the ST segment takeoff straightening in lead V2 and the ST segment coving in lead V1 are not seen in this previous ECG!
- Bottom Line: I still was not convinced that ECG #1 represented an acute OMI — but at this point in my analysis, I felt the following steps would be needed to rule out this possibility: i) Serial ECGs; ii) Serial Troponins; iii) Bedside Echo during CP (looking for a localized wall motion abnormality); — and, iv) Careful review of this patient’s chart regarding events of prior ED visits and hospital admissions, including documentation of any additional diagnostic studies that were performed.
= = =
Figure-1: The first 2 ECGs in today’s case.
= = =
Did YOU Notice the Increase in J Waves?
Although prominent J-point deflections are a common accompaniment of benign repolarization variants — J waves may occasionally be a marker of acute ischemia (See the Addendum to My Comment at the bottom of the page in the January 19, 2026 post).
- Documentation of J waves potentially serving as an ischemic marker has been noted in the literature (Andreou — Cardiol J 28(4):638-639, 2021 – and – Andreou — Eur Heart J Case Rep 6(7):ytac249, 2022).
- The mechanism for development of ischemic J waves is thought to relate to conduction delay in ischemic myocardium and accentuation of the potassium current-mediated action potential notch during early ventricular repolarization in epicardium but not endocardium.
- Ischemic J waves may increase in size if acute ischemia persists and/or worsens. J waves may decrease in size and/or disappear as CP and associated ST elevation resolve (as was seen in the January 19, 2026 post). And, the location of ischemic J waves may help to localize the “culprit” vessel.
- Clinically — Development of ischemic J waves has been shown to confer an increased risk of developing VFib (thought to reflect the increase in transmural dispersion of ventricular repolarization that these J waves serve as a marker for).
- Editorial Comment: I thought “Life was easier” before I learned about the existence of “ischemic J waves”. Overall, in my experience — this is a rare phenomenon, and I continue to associate the finding of J-point notching and terminal R wave slurring as common accompaniments of what usually ends up being a benign repolarization variant of ST elevation.
- BUT — When I see a decided increase in the number of leads with J-point notching, and in the size of these J-point deflections over the course of serial tracings recorded from a patient being evaluated for acute CP — I consider the possibility of ischemic J waves.
- As a result, adding to my potential concern regarding the findings in ECG #1 — I found it noteworthy that the number and size of J-point notchings were greatly increased when comparing today’s initial ECG with the previous ECG, as shown in Figure-1.
- Fortunately, as emphasized above by Dr. Smith — Chart review of today’s patient revealed a recent completely normal CT coronary angiogram — bedside Echo was totally normal without wall motion abnormality — and serial ECGs showed no evolution — allowing the safe conclusion of a Type-2 MI (due to supply-demand mismatch) accounting for modest Troponin elevation without the need for cardiac catheterization.
= = =
About CPAC ( = Cocaine-Associated Chest Pain):
I found the following 2 references insightful regarding the entity of Cocaine-Associated Chest Pain (Havakuk et al — JACC Archives 70(1):101-113, 2017 — and — McCord et al — Circ 117(14):1897-1907, 2008 ).
- Cocaine-related complications account for ~500,000 ED visits annually in the U.S. — with chest pain being the most common reason bringing these patients to emergency care.
- Despite this high number of ED visits — less than 6% of these patients with cocaine use end up having an acute MI confirmed by Troponin elevation. Thus, the great majority of patients we see who present with CP to the ED following cocaine use will not have an acute MI (and, as shown in today’s case — among those who do have an MI, supply-demand mismatch rather than acute coronary occlusion may account for a significant number).
- That said — interpretation of the initial ECG in such patients may be challenging, with a surprising number showing ST elevation due to the predominance of younger adult males among cocaine users, with this being the most likely group to manifest ST elevations from repolarization variants.
- The sinus tachycardia so commonly seen with acute cocaine use — is another potential contributor to ST elevation from myocardial demand ischemia (ie, rapid heart rates shorten the period of diastolic filling — while at the same time increasing oxygen demand).
- The mechanisms for cocaine-induced adverse cardiovascular effects are multiple: i) Increased sympathetic activity (with resultant tachycardia, increased blood pressure, enhanced cardiac contractility); — ii) Coronary vasoconstriction (alpha-adrenergic stimulation; impaired nitric oxide [vasodilator] production; increased endothelin-1 levels); — and, iii) Prothrombotic effect (increased platelet activity and aggregation; increased plasminogen activator inhibitor activity).
- Bottom Line: Chest pain following acute cocaine use is a common cause of ED visits. Although the vast majority of these patients will not have acute coronary occlusion (ie, many have supply-demand mismatch or non-cardiac causes of their CP) — cocaine use is notorious for its multifaceted adverse cardiovascular effects, which include thrombotic predisposition that can on occasion result in acute OMI. Therefore — a prudent approach is warranted until an acute cardiac event can be confidently excluded (which fortunately was possible in today’s case!).
= = =
= = =