This case was contributed by Brooks Walsh, an ECG enthusiast who has contributed frequently, and edited by Smith
Case
An
elderly male called EMS after he developed “indigestion.” The paramedic
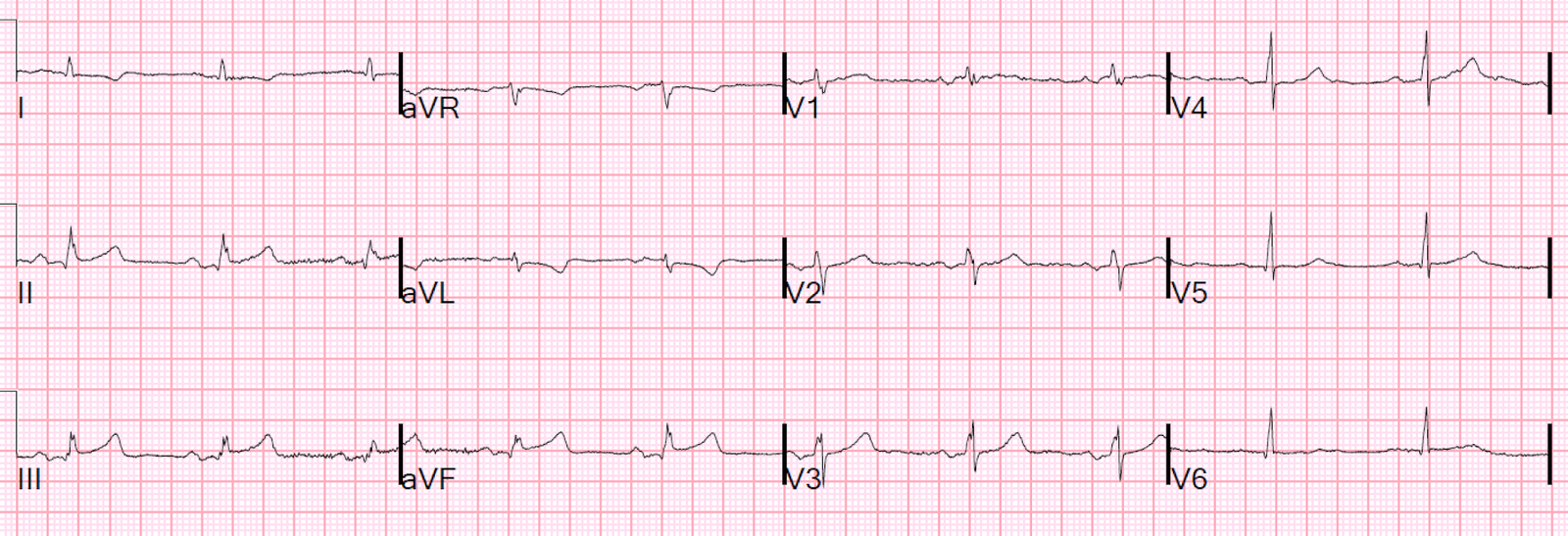
recorded a series of ECGs; the initial ECG is representative here:
 |
|
Computer read: “Normal ECG” What do you think?
Algorithm is either Glasgow or Marquette 12 SL |
This ECG is diagnostic of LAD occlusion because of terminal QRS distortion in lead V3. See explanation below.
Smith sent this to the Queen of Hearts years later. Here is the result:

The Queen of Hearts PM Cardio App is now available in the European Union (CE approved) the App Store and on Google Play. For Americans, you need to wait for the FDA. But in the meantime:
YOU HAVE THE OPPORTUNITY TO GET EARLY ACCESS TO THE PM Cardio AI BOT!! (THE PM CARDIO OMI AI APP)
If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list.
https://share-eu1.hsforms.com/18cAH0ZK0RoiVG3RjC5dYdwfyfsg
Two
doses of nitroglycerin reduced the patient’s symptoms during transport.
He was almost asymptomatic when he arrived in the ED. The paramedic
interpreted this as a STEMI.
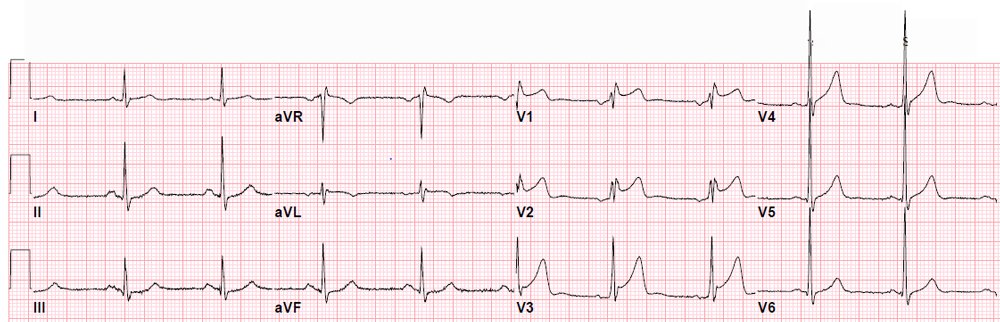
An ECG was obtained in the ED:
 |
There is ST elevation in V2-V4. Is it normal ST elevation (early repol?) or LAD occlusion?
The computer read this as “Early repolarization, otherwise normal ECG.”
What to you think?
Comment: the T waves in V2 and V3 are massive compared with the R waves, nearly diagnostic of hyperacute T waves.
Can you employ the Subtle Anterior STEMI calculator?
The
Subtle STEMI calculation is used to differentiate a subtle anterior
acute coronary occlusion from early repolarization (ER). ER is
unlikely, given the age, but there is STE in both the anterior and
lateral leads, and the J-points are either notched or slurred in many of
those leads. Also, the STE is concave-upwards, further supporting ER as
a “STEMI-mimic” in this case, though in approximately 40% of acute LAD occlusion, upward concavity is present in all of leads V2-V6.
Use of calculator (formula) on the EMS 12-lead: The EMS 12-lead had QTc 401 ms, with STE60V3 of 2.0 mm, and RA in V4 of 18 mm, resulting in a value of 20.2. (Even making STE60V3 = 3.0 mm, and RA in V4 15 mm only moves the result to 22.4.)
Thus, using the Subtle Anterior STEMI calculator, the EMS ECG is strongly predicted to be ER, while that in the ED is borderline, and changed markedly depending on the baseline used in V3.
How about using the calculator on the ED 12-lead?
The ED ECG is more equivocal.
The QTc 439 ms, with STE60V3 of 2.0 mm, and RA in V4 of 16 mm, resulting in a value of 23.1 However, even small changes in RV4, and especially in V3STE60, tilt the result on ether side of 23.4!
However: one should not use the calculator in this patient!
The patient has overt evidence of anterior acute coronary occlusion, and so the formula might provide false-negative results.
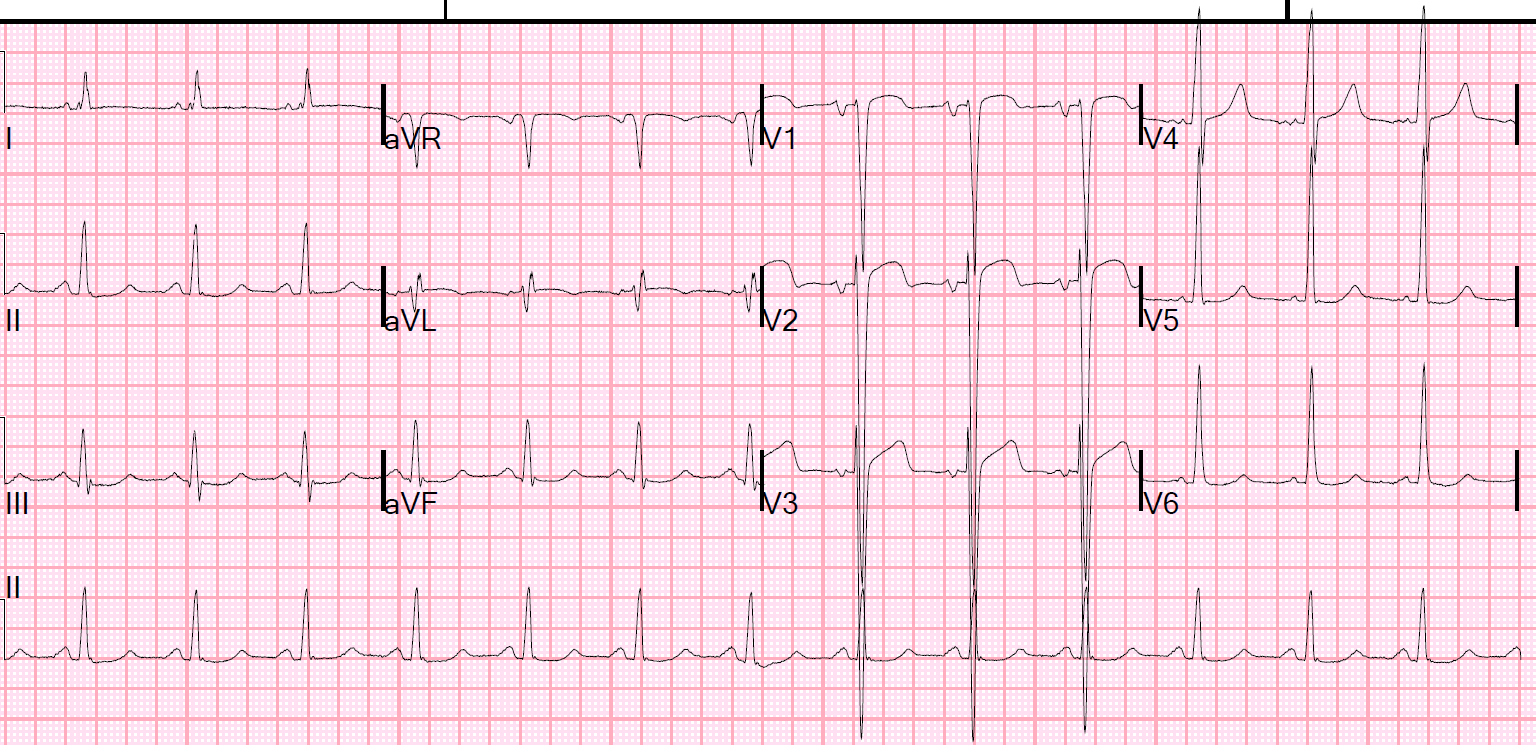
In this case, there is “terminal QRS distortion,” which in our study was a sign of “obvious” MI and thus an exclusion. We have studied this (will be published) and found that it does not occur in early repol.
Terminal QRS distortion was defined as the absence of both a J-wave and an S-wave in either of V2 or V3. In this case (see image below), there is virtually no S-wave in lead V3, nor is there a J-wave. The EMS 12-lead shows that the S wave (blue arrow) does not descend below baseline. The ED 12-lead, obtained in the context of improving symptoms, shows an S wave (red arrow) that just barely dips below the baseline.
 |
|
This is terminal QRS distortion, and it has been discussed before here and here. |
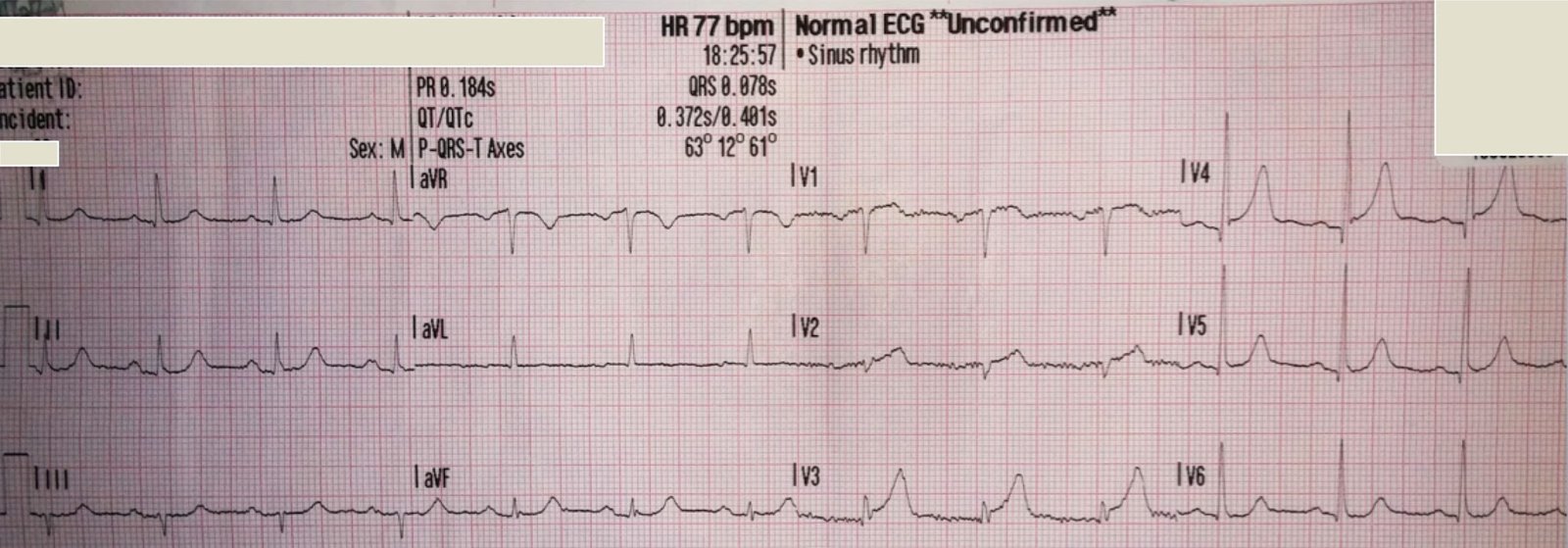
An ECG was found from 2 months prior:
 |
| There is no ST Elevation, normal R- and T-waves, normal S-waves in V2 and V3. |
The
old ECG served as confirmation, but was not necessary to activate the
cath lab.
Pretest Probability
In a recent case with marked ST elevation, I argued that the pretest probability was low and one should therefore investigate more before activating the cath lab. In that case, the patient did not have chest pain but was 36 years old. This patient does not have chest pain but is elderly and that increases the pretest probability by a huge amount. Furthermore, because of terminal QRS distortin, this ECG cannot be early repolarization, whereas that previous ECG with approximately 5 mm of ST elevation was indeed due to early repol.
Additionally, a bedside echo was performed while waiting for the cath lab team to arrive, and it showed characteristic hypokinesis of the LAD distribution (apex and distal septum) on the apical 4-chamber view:
Outcome:
The cath lab was activated and a 99% LAD obstruction was found and opened and stented