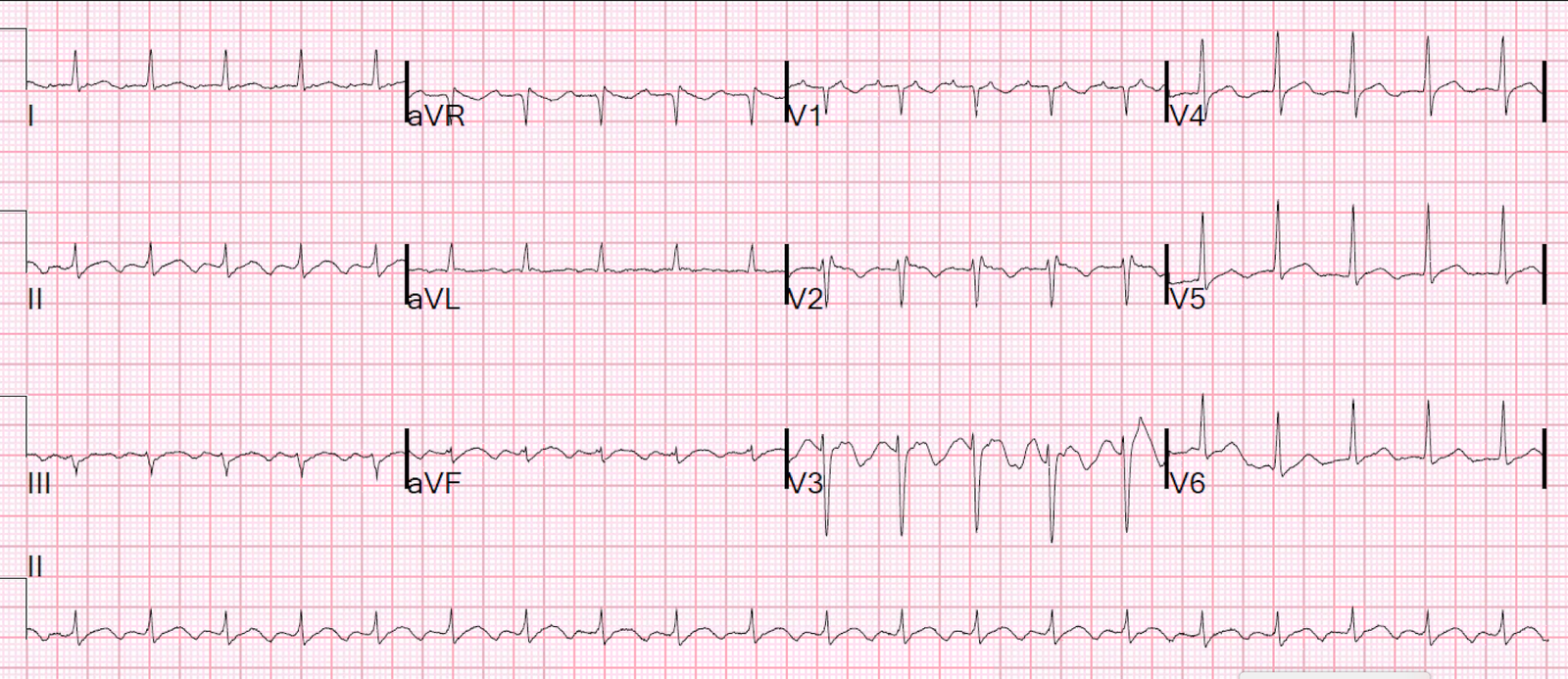
A 50-something presented with bradycardia. No other history is available. Here is the EKG:
 |
| There is obvious atrial flutter. The ventricular rate is 29. The QRS has the morphology of Right Bundle Branch Block (RBBB) and Left Anterior Fascicular Block (LAFB) There is also a very long QT, primarily due to a long ST segment |
This is NOT really RBBB and LAFB. The flutter waves are not conducting through the AV node. This is not Flutter with 7 or 8 to 1 conduction. Instead, there is third degree (complete) AV block.
How do I know? When atrial flutter conducts, the QRS should occur at the same part of the flutter wave for every QRS. Every time the flutter circuit goes around the atrium it arrives at the AV node at the same part of the wave and, if the AV node is ready to conduct, that is when it conducts.
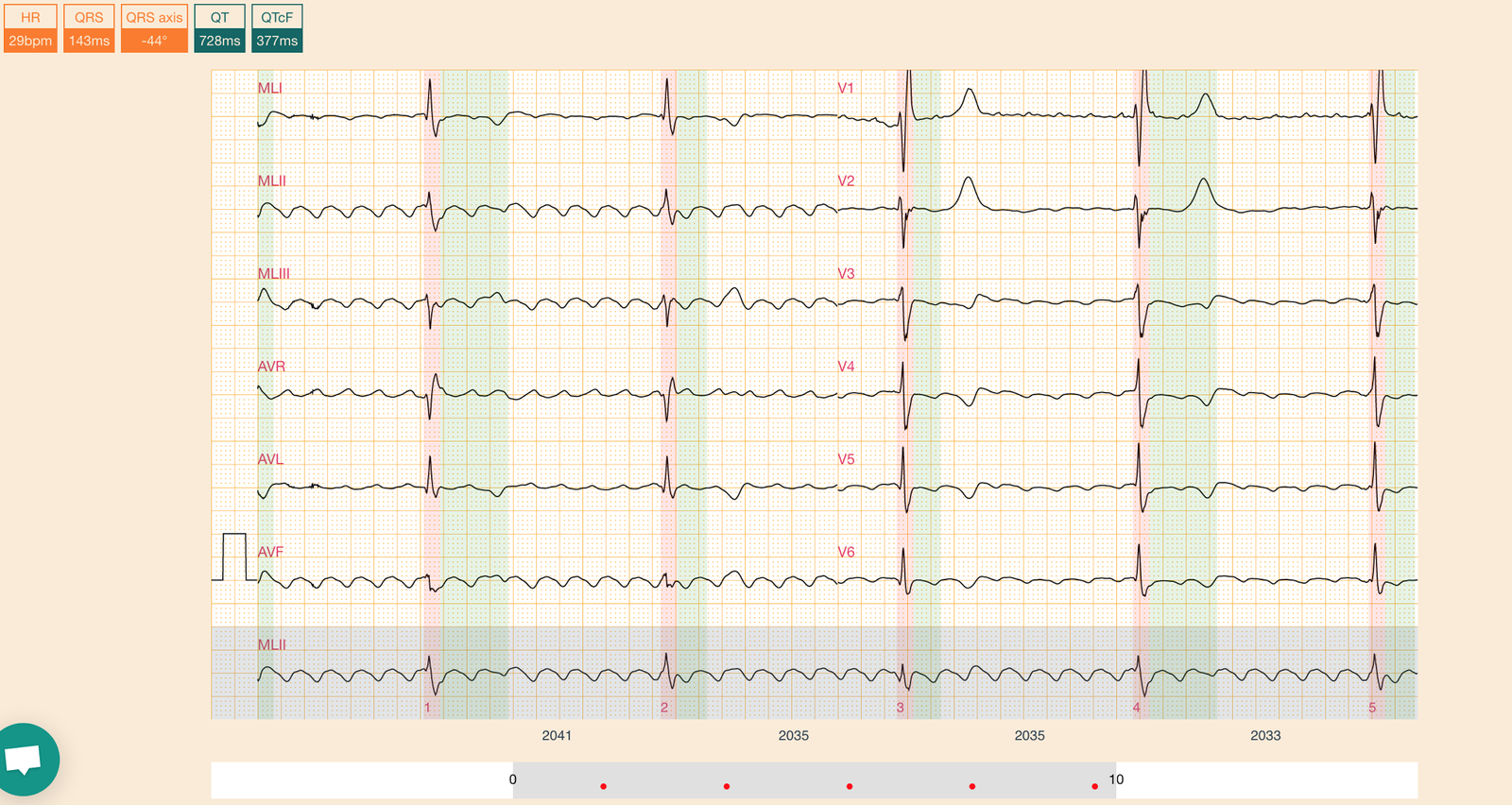
If you look closely, this does not happen:
 |
| On beat 1, the QRS starts at the peak. On beat 2, it starts earlier On beat 3, it starts earlier still On beat 4, it starts just after the peak Beat 5 looks like beat 2. Instead, there is a very regular escape rhythm |
Thus, there is complete AV dissociation.
[There are times when there is atrial flutter and Wenckebach, and the lengthening PR interval changes this otherwise fixed relationship between flutter waves and QRS, but it is far more rare than complete block AND it does not occur with 6:1 block.]
So this is atrial flutter with complete AV block and a regular escape rhythm.
Is it a junctional escape? A junctional escape should be around a rate of 40, and it should be narrow, unless there is a junctional escape + RBBB + LAFB. This is possible.
Much more likely is that this is a ventricular escape. Then why the RBBB and LAFB morphology? Because the escape is originating in the posterior fascicle. When there is a supraventricular rhythm with RBBB and LAFB, the impulse gets to the posterior fascicle only, then spreads to the ventricle from the posterior fascicle. Thus, RBBB + LAFB also, in a sense, originates from the posterior fascicle. In this case, there is no supraventricular stimulus. There is only the automatic escape, and it originates from the posterior fascicle.
Diagnosis: Atrial Flutter with complete, third degree, AV block. The long ST segment is probably due to hypocalcemia. Consider hyperkalemia.
Consider reversible causes (especially hyperkalemia or drug effect from beta blockers or calcium channel blockers before pacing).