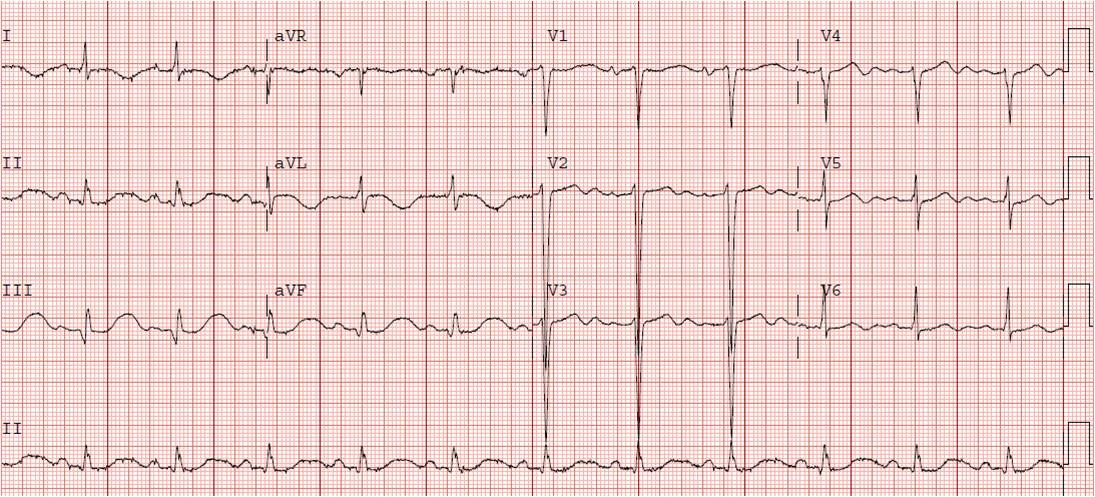
The computerized QTc is 472, but the actual QTc is well over 600 ms. The T-waves are almost like a sine wave, and there are very prominent U-waves, best seen in precordial leads. These findings are pathognomonic of hypokalemia, and this was indeed the etiology of the cardiac arrest.