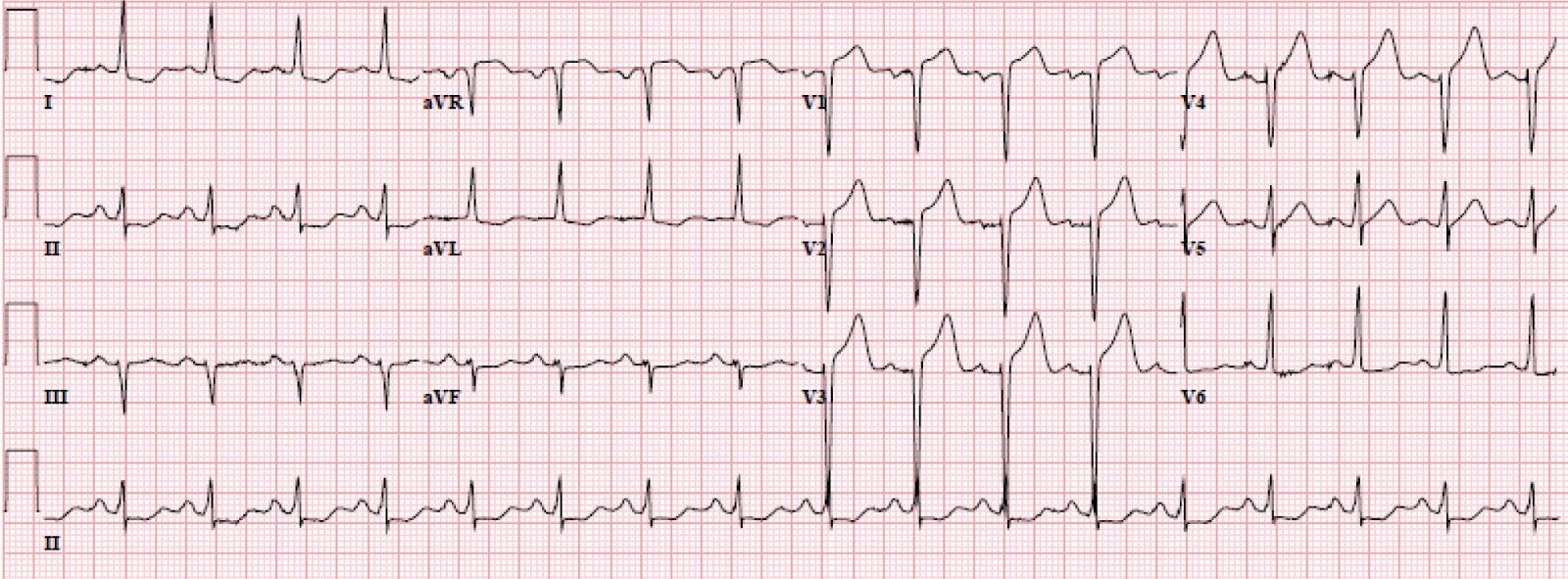
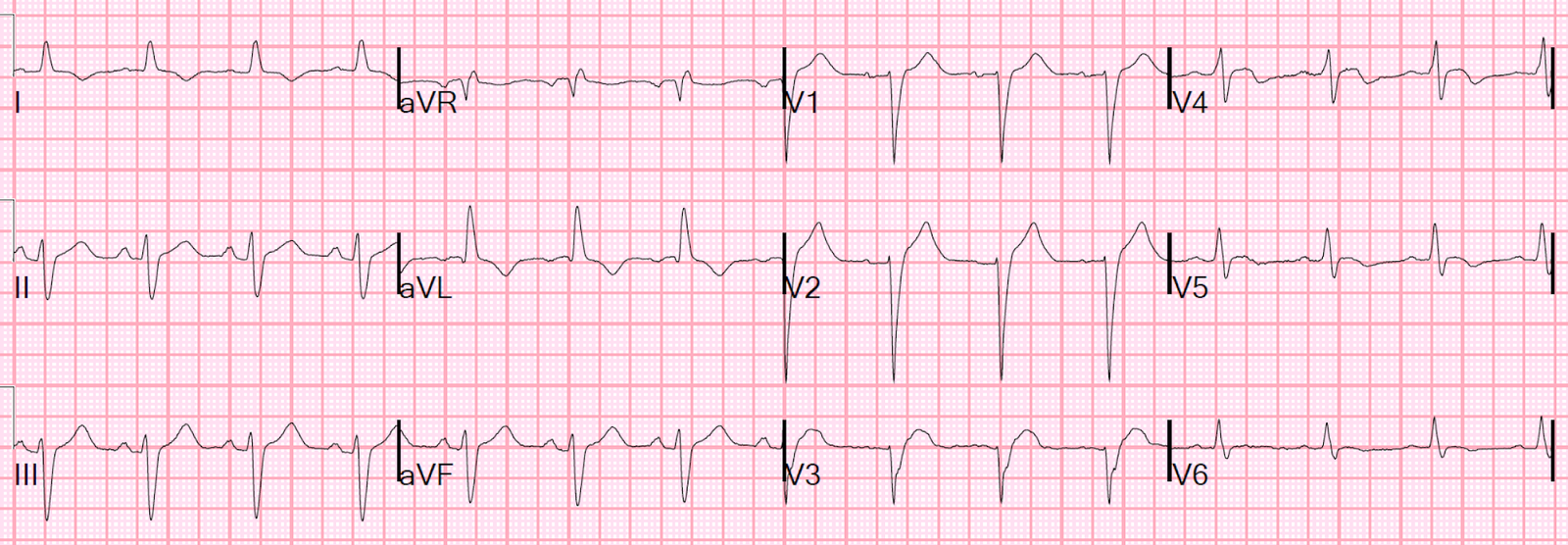
An elderly male presented with 48 hours of off and on chest pain. This ECG was recorded with pain:
 |
| The QRS is 130 ms. It is essentially LBBB, though some might quibble with the tiny Q-wave in aVL or the fact that the intrinsicoid deflection (onset to peak of R-wave in V5, V6) is not quite 60 ms (it is at least 55 ms). When I first glanced at this, I did not think it looked like STEMI (that is, I did not think it met the modified Sgarbossa criteria) |
But then I measure it. Here is V3 magnified:

Here I point out where the J-point and the PQ junction are:
 |
| You can see that, no matter which complex you measure, the ST elevation at the J-point is at least 3.5 mm. The S-wave is no more than 13 mm. Thus, the ST/S ratio in V3 is greater than 0.25. There is thus proportionally excessively discordant ST elevation. Only one lead is required! |
The cath lab was activated.
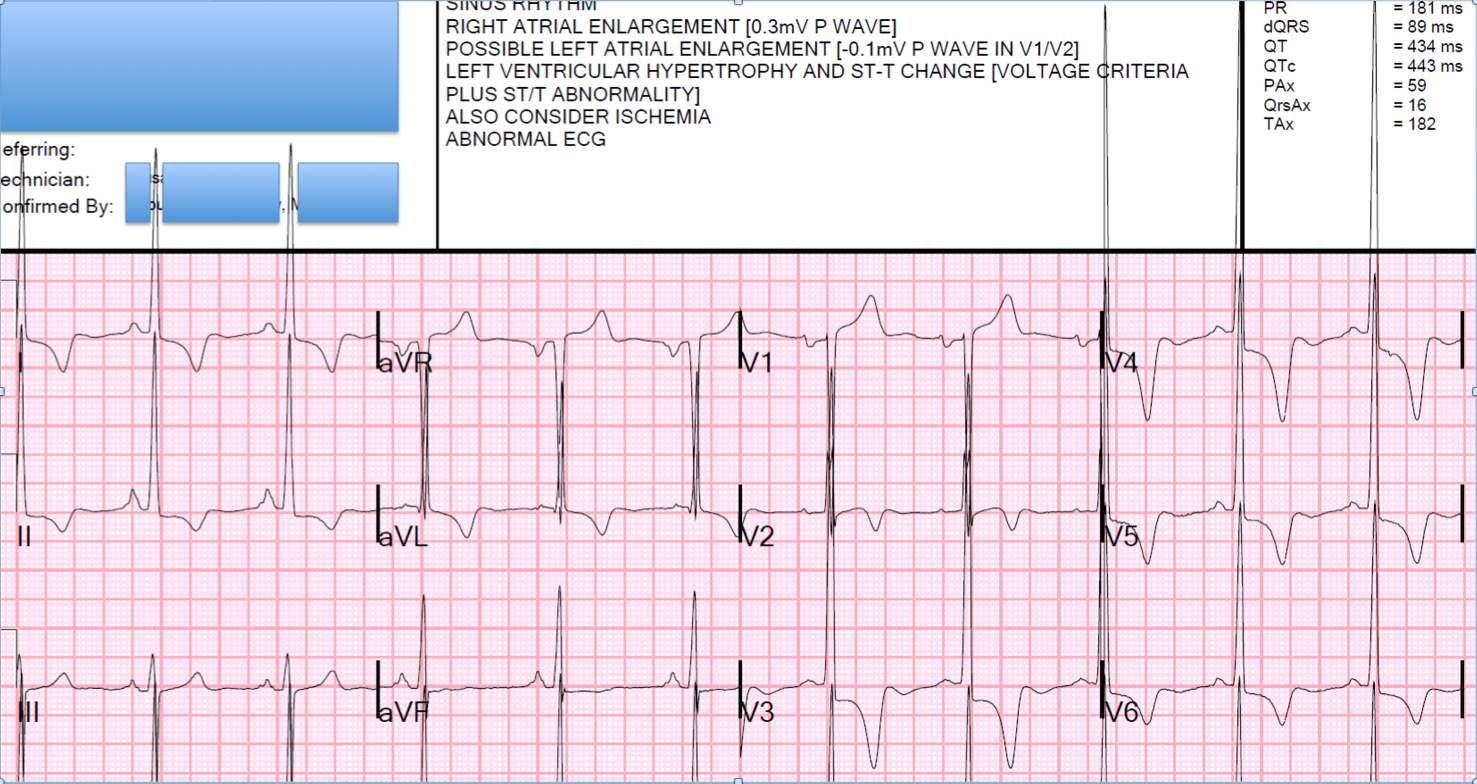
Another ECG was recorded, with reportedly ongoing chest pain:
 |
| Now the ST elevation is less. The ratio is about 3/15 = 0.20. 0.20 is still very good for diagnosing coronary occlusion. However, look at lead V4: there is 1.5/5.0 = 0.30 ratio (the QRS is so different from the first ECG that I suspect some lead placement changes) This improving ECG makes it appear as if there is some reperfusion of the artery. |
At angiogram, a 90% thrombotic lesion was found and stented. I suspect that the artery had spontaneously reperfused prior to the angiogram. That is why the ST segments were falling.
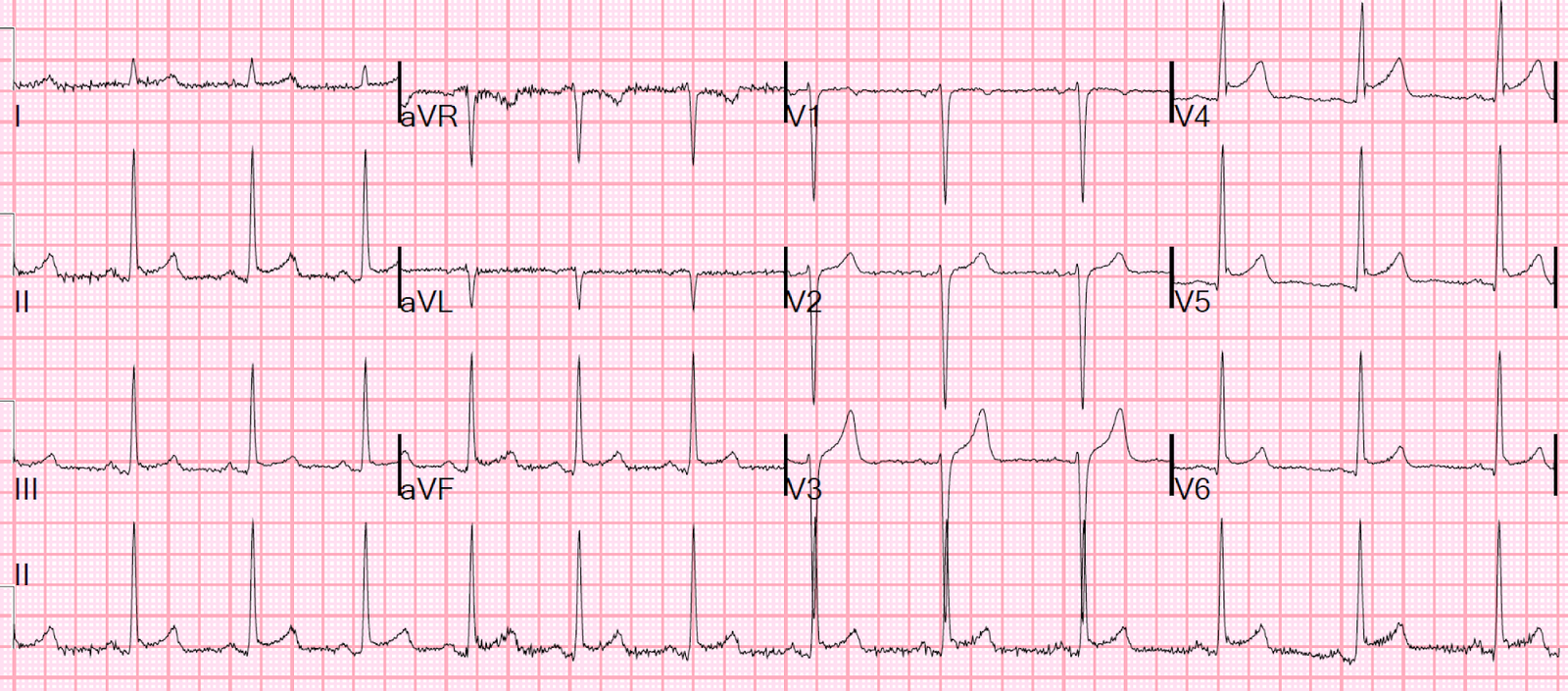
Here is the post-PCI ECG:
 |
| It is now much more atypical for LBBB and should be called a nonspecific intraventricular conduction delay. QRS is 126 ms. The disproportionally excessive discordant ST elevation is gone. |
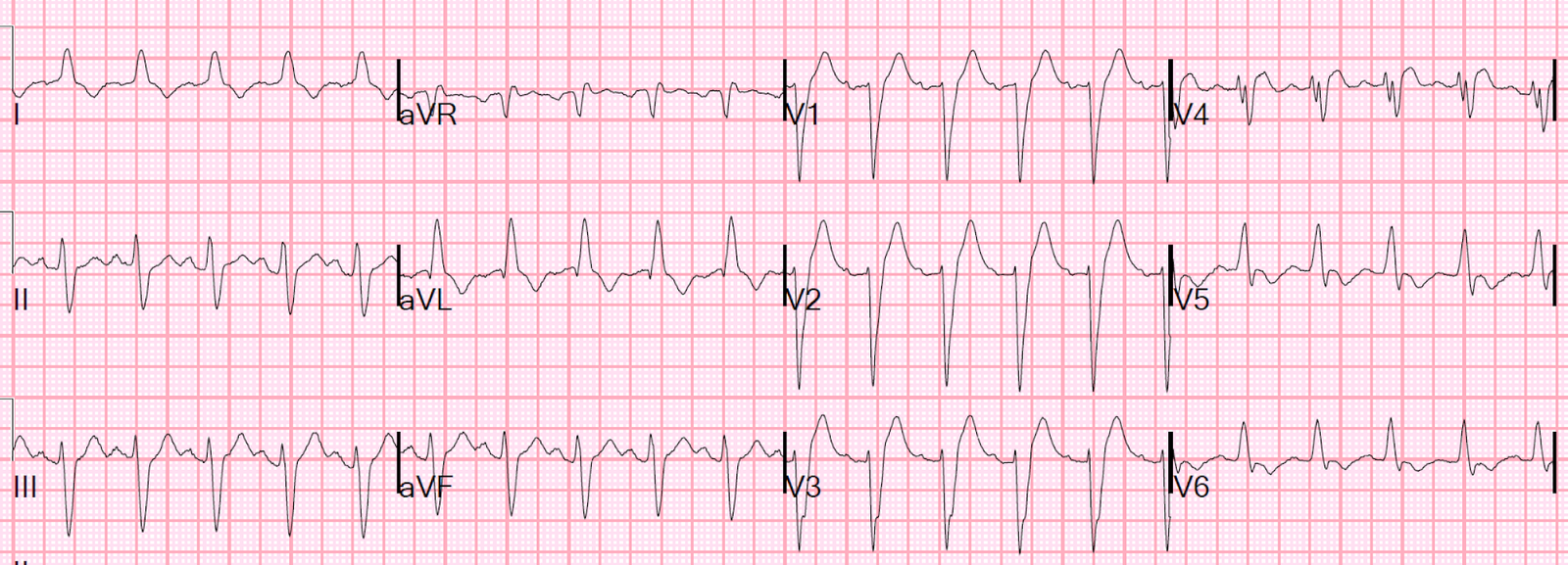
This is 2 days later:
 |
| LBBB is gone. There is normal conduction and anterior reperfusion T-waves. |
Learning Point:
In LBBB, measure the ST elevation at the J-point and the PQ junction. In a patient with the right clinical scenario, if there is one lead with a ratio greater than 0.25, then there is occlusion until proven otherwise.