







Early Repolarization vs LAD Occlusion
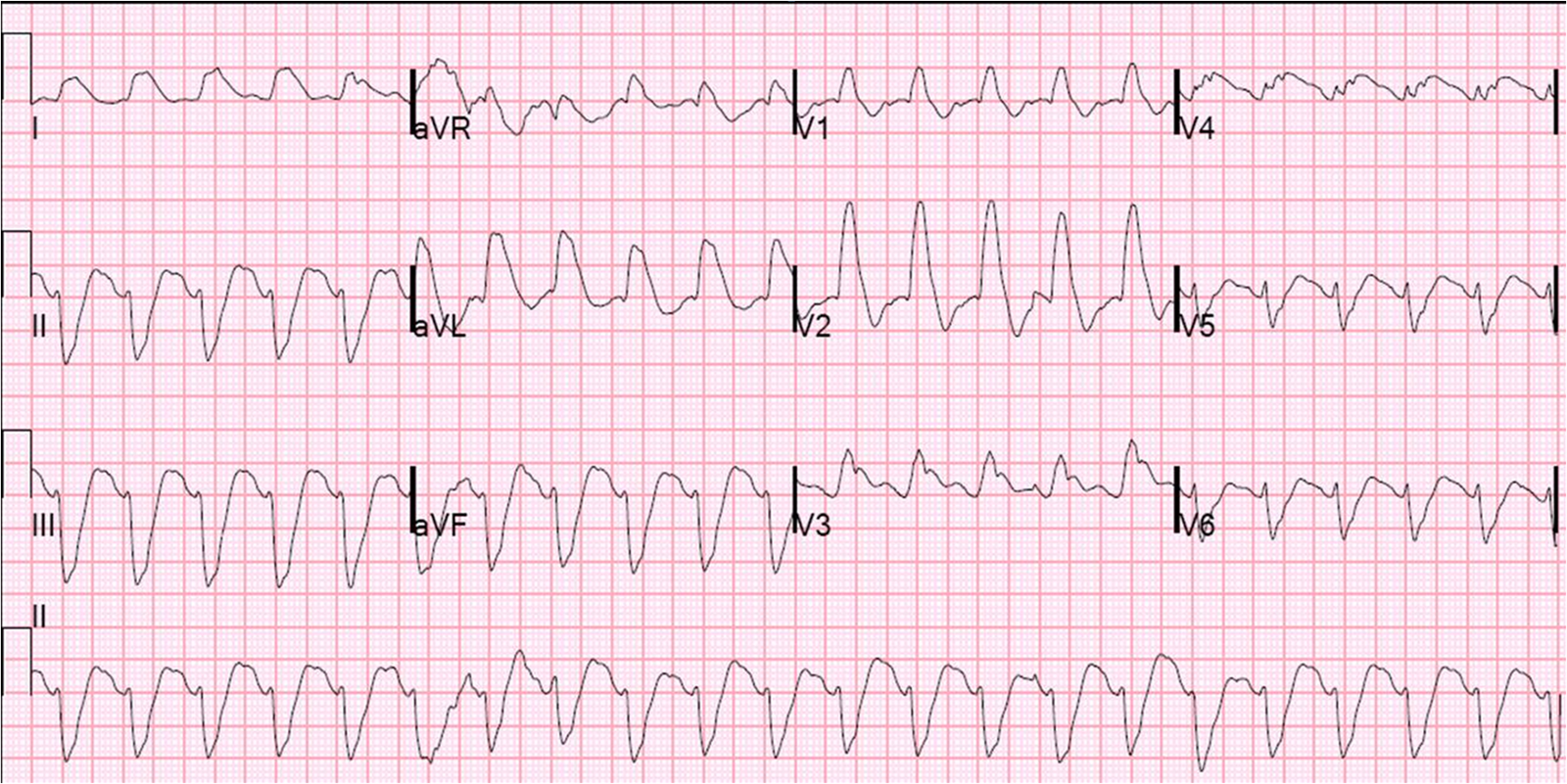
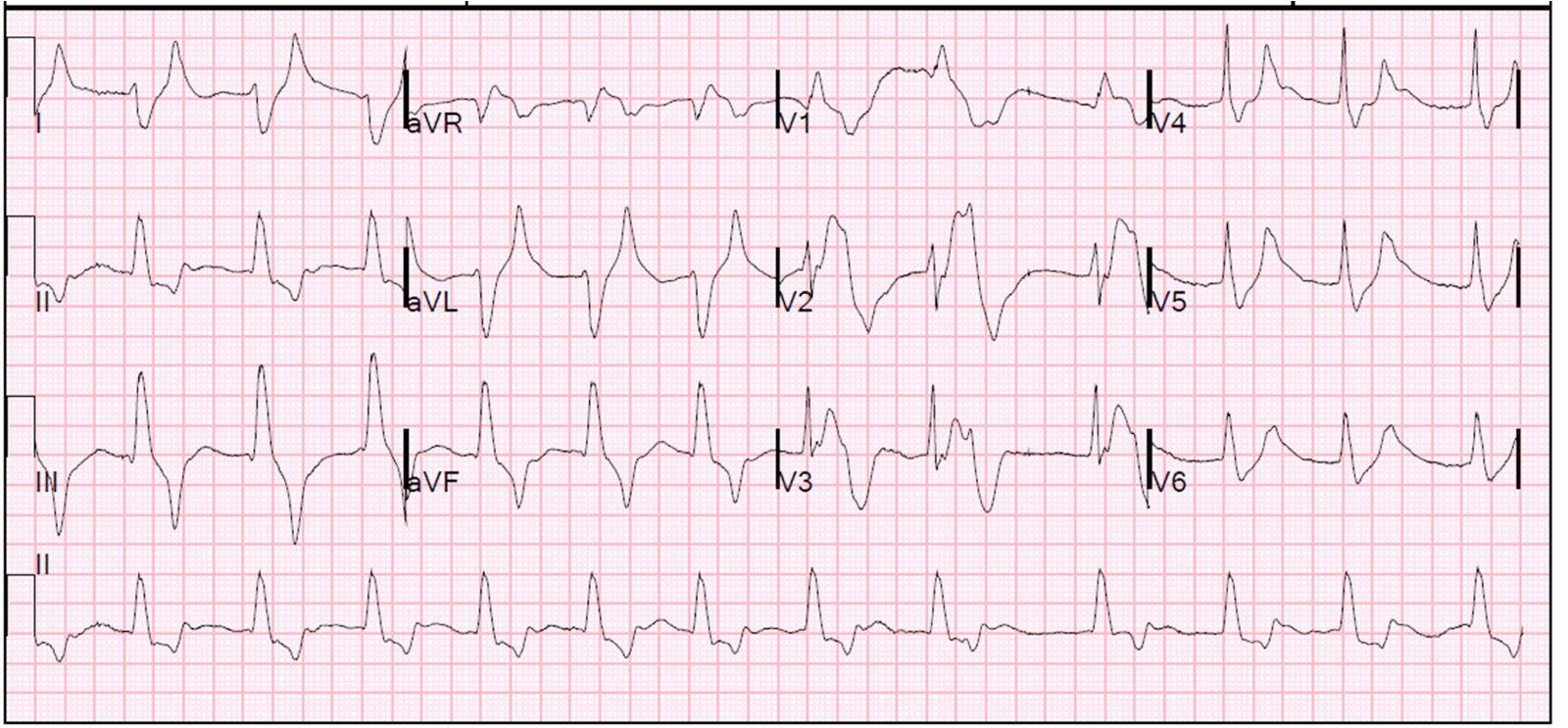
First ECG in Video 2nd ECG in Video
Associate Editors:
— Pendell Meyers & Ken Grauer (2018)
— Jesse McLaren & Emre Aslanger (2022)
— Willy Frick (2024) — Sam Ghali (2025)