A 33 year old male had 2 days of chest pain, intermittently relieved with acetaminophen (paracetamol) and diclofenac. He came to the ED after 5 hours of constant chest pain. He had a possible history of fever.
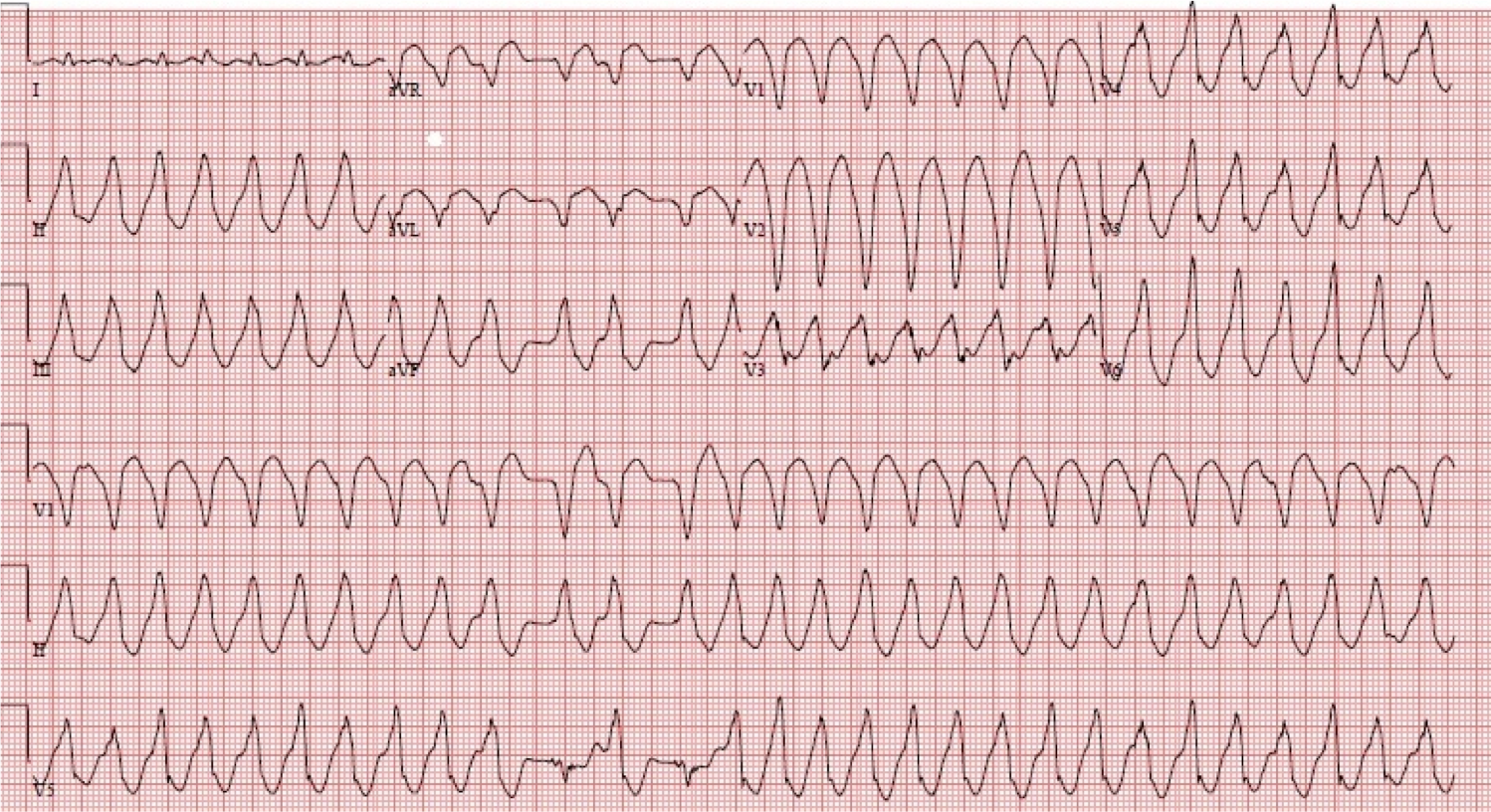
He had this initial ECG:
 |
| The leads on the right are, from top to bottom: I, II, III, aVR, aVL aVF. There is ST elevation in anterior leads. as well as lateral and also inferior. There are also QS-waves in anterior leads, suggesting that this is a well developed infarct. |
The diffuse ST elevation led the emergency physician to believe that this might be Takotsubo Stress Cardiomyopathy. He also thought, due to the fever, that it might be myo-pericarditis. So he did a bedside echo:
Keep watching, there are several views:
The base of the heart has excellent concentric function, but the apex is “ballooning:” the entire apex functions poorly. This is typical of takotsubo (the name refers to a Japanese octopus trap which has a narrow mouth and ballooning apex so that an octopus cannot escape it). These images confirmed his suspicion that this diffuse ST elevation was due to takotsubo.
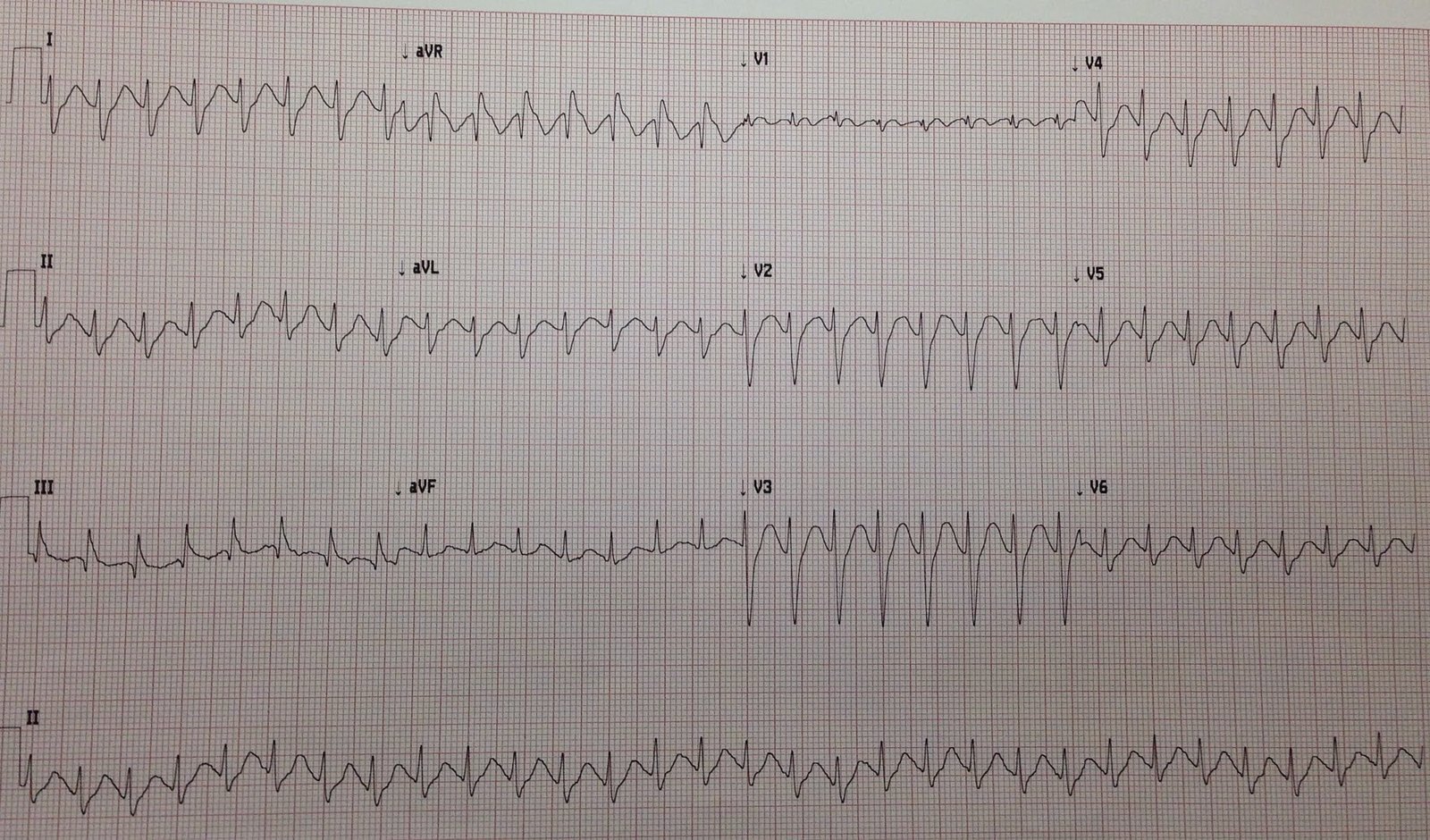
He recorded another ECG 2 hours later:
 |
| There is less ST elevation now. |
At this point, he decided to send the patient to a PCI facility, just in case.
He immediately sent me these ECGs and the echo and asked my opinion.
I responded that there is far too much ST elevation for this to be Takotsubo. That, by ECG, this is a proximal occlusion of a “wraparound” LAD that supplies not only the anterolateral walls, but the inferior wall. So it is an anterior/inferior/lateral STEMI. As for the ultrasound, it
is strange that there is not more wall motion abnormality. So of
course takotsubo is on the ddx. But the apex reflects all 3 walls too.
This is STEMI, not Takotsubo.
“What was the outcome?”
Answer:
Yes.. I got the results
It was proximal wraparound LAD, stented..
It seems the ECG alone is enough
And echo might confuse the picture
Thanks again
CK 3300 CKMB200 trop 35
Kosuge et al. http://content.onlinejacc.org/article.aspx?articleid=1204510, found that ST depression in aVR combined with absence of ST elevation in V1 was highly predictive of Takotsubo vs. LAD occlusion. If this rule had been followed, it would have been wrong! It is an exception to the rule.
Learning Point:
There is more to assessing the ECG that this simple rule. Takotsubo and LAD occlusion can exactly mimic each other. Just be the height of ST elevation, I could tell this was NOT Takotsubo, in spite of the echo and the ECG rule.