A male in his 40’s was discharged from the ED after evaluation for chronic back pain. He was denied opiate medication and was very upset with this. Shortly after discharge, he developed acute chest pain, diaphoresis and pre-syncope. EMS was called and they recorded a BP of 50. They recorded this ECG:
 |
| Sinus rhythm with diffuse ST elevation (anterior, inferior, lateral) and hyperacute T-waves, diagnostic of subepicardial ischemia. The differential diagnosis is occlusion of a wraparound LAD that feeds the anterior/inferior and lateral walls vs. Stress cardiomyopathy causing similar ischemia of all these territories. |
The medics activated the cath lab prehospital.
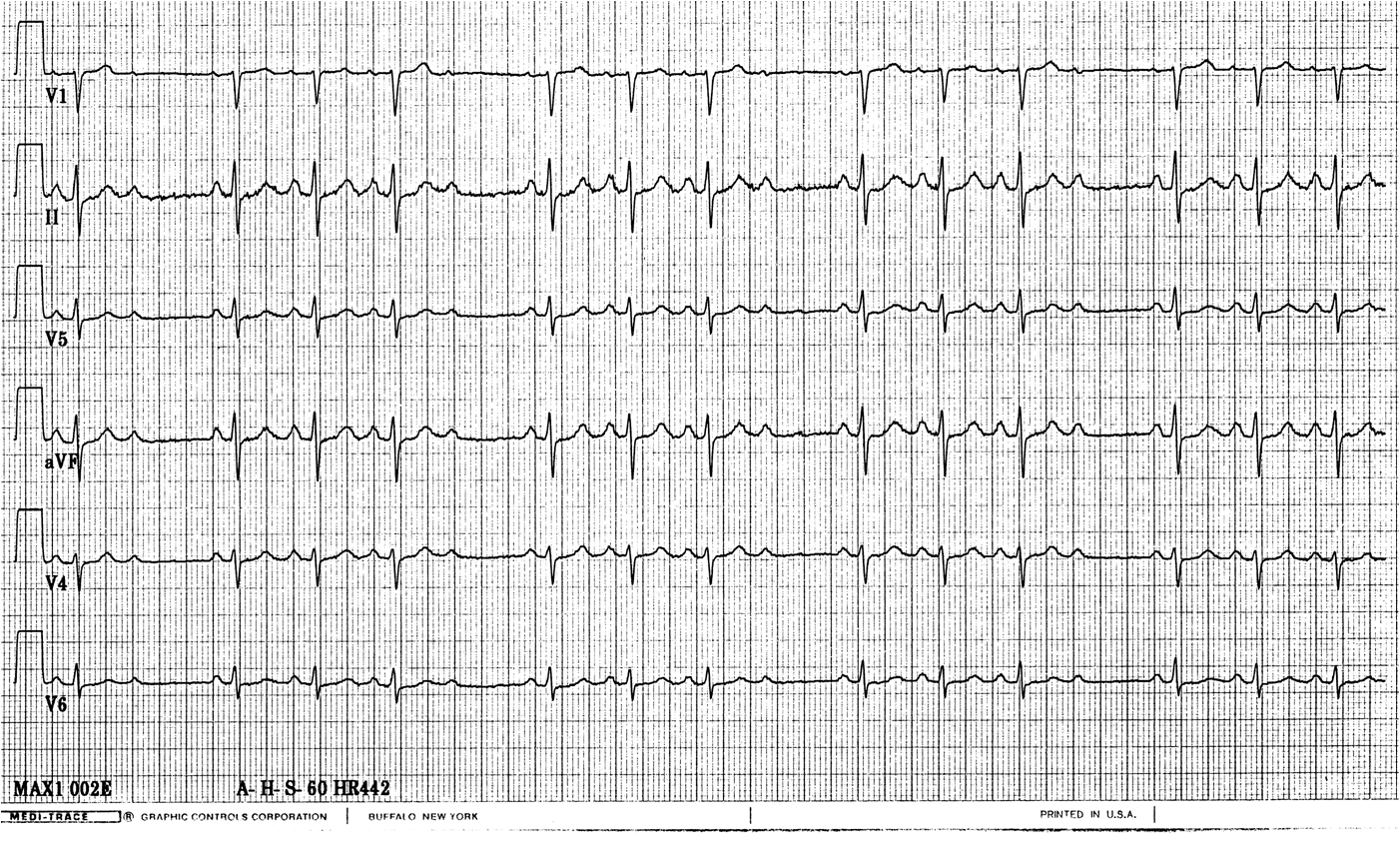
He arrived in the ED tearful and agitated and required much consoling. His coronary risk factors were smoking and hypertension. This ECG was recorded at time zero:
 |
| No significant change |
Here is his previous ECG:

A bedside echocardiogram showed poor function, but was not more specific. The patient took prolonged persuasion to consent to going to the cath lab.
This ECG was recorded at time 30 minutes:
 |
| The hyperacute T-waves are resolving, as is the ST elevation. The ischemia is greatly improving. |
The patient was taken to the Cath Lab and found to have no significant coronary disease. Troponin I peaked at 0.3 ng/ml. A formal echocardiogram showed severely decreased LV systolic function with the estimated left ventricular ejection fraction at 20-25 %. There were wall motion abnormalities in mid to distal LV wall segments, with sparing of the basal LV segments, all highly suggestive of Takotsubo type stress induced cardiomyopathy.
How to suspect takotsubo stress cardiomyopathy from the presenting symptoms, signs and ECG
First,
it is believed to by caused by diffuse small vessel ischemia due to
catecholamines, and thus has the same electrophysiologic substrate as
STEMI. It affects the entire heart except the base, resulting in diffuse circumferential wall motion abnormalities that only spare the base (top) of the heart. These diffuse wall motion abnormalities (lateral,
posterior, inferior, septal, anterior, apical) result in systolic “apical
ballooning” which looks like a Japanese octopus trap (a takotsubo).
Of course, the clinical presentation can help to suspect this: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3214344/
It
is most common in postmenopausal women and is associated with severe
emotional upset (stress) or severe physiologic stressors such as
respirtory failure.
Stress Cardiomyopathy (Apical Ballooning syndrome, or Takotsubo cardiomyopathy) only presents with ST elevation in about 1/3 of cases, but when it does, it is one of the most difficult mimics of anterior STEMI, and often the only way to tell the difference is to do an angiogram.
ECG Differentiation
A review and analysis of the literature in ECG differentiation of the two entities (1-6) reveals that an analysis of ST elevation vector is a good predictor of anterior STEMI vs. stress cardiomyopathy. In anterior STEMI, whether proximal, mid, or distal LAD occlusion, there is ST elevation in V1 (1 mm measured at 80 ms after the J-point) in about 80% of cases, whereas this is present in 20% of cases of SCM. SCM also has a negative ST segment in aVR and is more likely to have ST elevation in inferior leads, or at least absence of ST depression in inferior leads (however, 40% of anterior STEMI lack inferior ST depression). Finally, precordial ST elevation in SCM is more pronounced in V3-V5 vs. V2-V4.
Putting these all together, it is apparent that the ST vector in anterior STEMI is more commonly anterior and superior (V1-V4), without STE in inferior leads, whereas in SCM the ST Vector it is more inferior and lateral (V2-V5, with STE in inferior leads and ST depression in aVR). This correlates with the location of wall motion abnormalities in SCM (diffuse and toward the apex, similar to pericarditis, including inferior and lateral walls) vs. anterior STEMI (anterior as well as septal-apical).
This Case
1. The patient was very stressed and emotionally upset and had just been denied opiates for his pain
2. There is diffuse ST elevation: anterior, inferior and lateral. Of course this could be a proximal LAD occlusion with a wraparound LAD such that all 3 walls are supplied by the LAD.
3. Absence of ST elevation in lead V1
4. ST depression in aVR
Final Assessment:
One might do a formal echo to look for apical ballooning, and this may help in diagnosing Takostubo, but given the present state of the art, I do not believe that there was enough information to confidently exclude anterior STEMI (LAD occlusion) based on clinical, ECG, and echo characteristics without doing an angiogram.
1.
Tamura
A et al. A New Electrocardiographic
Criterion to Differentiate Between Takotsubo Cardiomyopathy and Anterior Wall
ST-Segment Elevation Acute Myocardial Infarction. Am J Cardiol Sept 2011; 108(5):630-633.
2. Ogura
R, et al. Specific findings of the standard 12-lead ECG in patients with “takotsubo” cardiomyopathy: comparison with the findings of acute anterior myocardial infarction. Circ J 2003;67:687–
690.
3.
Inoue
M, et al.
Differentiation between patients with takotsubo cardiomyopathy and those with
anterior acute myocardial infarction. Circ J 2005;69:89 –94.
4. Bybee KA, et al. Electrocardiography cannot reliably differentiate transient left
ventricular
apical ballooning syndrome from anterior ST-segment elevation myocardial infarction. J Electrocardiol 2007;40:38.e1–38.e6.
5. Jim MH, et al. A new ECG criterion to identify takotsubo cardiomyopathy from
anterior
myocardial infarction: role of inferior leads. Heart Vessels 2009;24:124–130.
6. Kosuge M, et al. Simple and accurate electrocardiographic criteria to differentiate
takotsubo
cardiomyopathy from anterior acute myocardial infarction. J Am Coll Cardiol 2010;55:2514 –2516.
http://content.onlinejacc.org/article.aspx?articleid=1142882