This was a very interesting case:
A Very Fast Regular Narrow Complex, Followed by an Equally Fast Regular Wide Complex
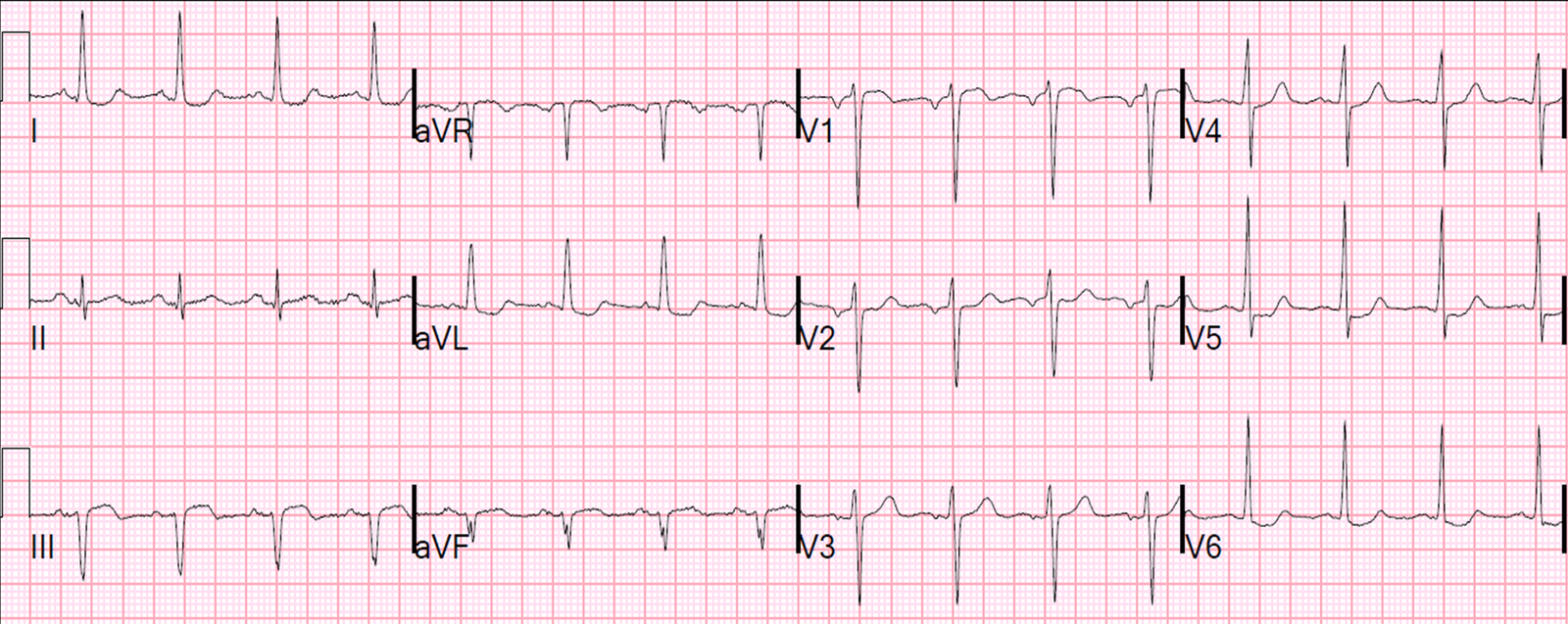
It had a very fast narrow complex rhythm, then a very fast wide complex rhythm, then converted to sinus with a very short PR interval.
We surmised that there must be accelerated AV conduction AND an accessory pathway.
The EP results are back, and:
1. Accelerated AV conduction
2. Left lateral accessary pathway. It was ablated.