This case was sent to me by for analysis by Scott Flannagan in Australia. I am by no means a rhythm master like Dr. K. Wang, but I think I was able to figure this one out. If anyone has a better idea, let me know. He will be able to get me the electrophysiology results in a few weeks, but I couldn’t wait to post it now.
Case
A young woman in otherwise excellent health presented with one year history of intermittent palpitations. She was alert but not well perfused: she had cool skin but she had no chest pain and was not diaphoretic. Her BP was 110/90.
Here was her 12-lead:
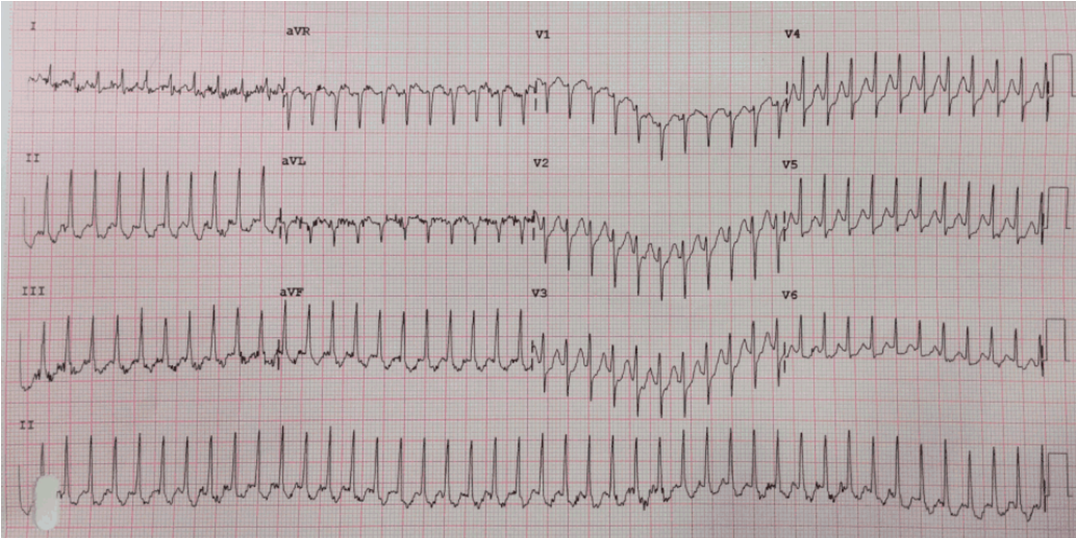 |
| There is a narrow complex, regular tachycardia that is very fast, at 259 BPM. Computerized QRS duration in 94 ms. |
No matter what is causing this, the rate is extremely fast and suggests remarkably fast AV nodal conduction. Children and infants can normally conduct this fast through the AV node, but not adults.
ECG Differential Diagnosis includes:
Paroxysmal SVT
—AV nodal re-entrant tachycardia vs.
—Orthodromic re-entrant tachycardia through a bypass tract (accessory pathway)
–If there are P-waves: Very fast Atrial Tachycardia with Very Fast AV conduction
Slow atrial flutter (rate 259) with 1:1 conduction through a fast conducting AV node
Every possibility includes very fast AV node conduction.
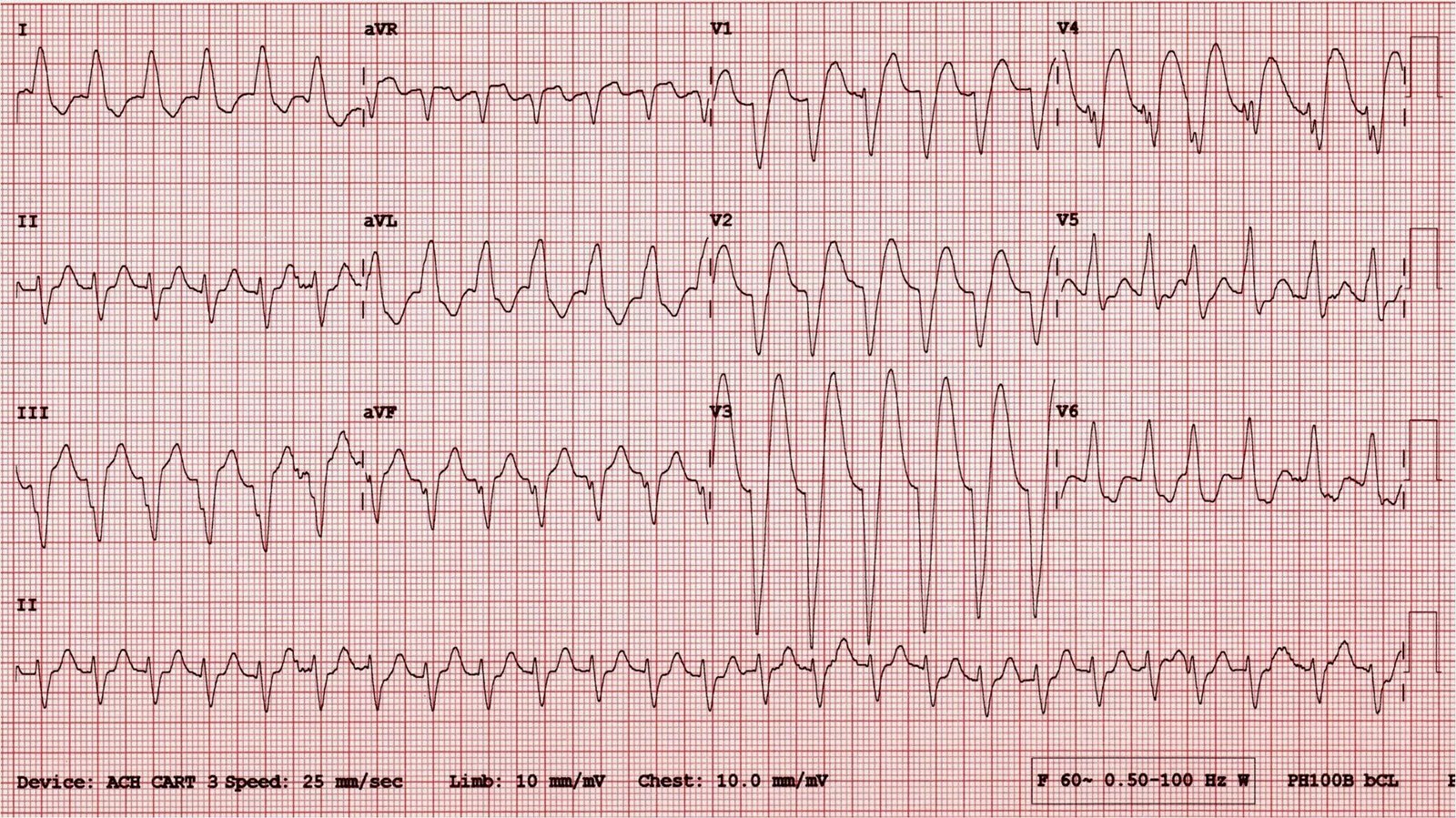
Pads were placed and the patient was given 6 mg of adenosine. Here is the subsequent 12-lead ECG:
 |
| Now there is a wide complex rhythm with a rate of 257 (essentially the same rate). Computerized QRS duration is 112 ms. Lead V4 gives the suggestion that there is no wide complex, but rather a narrow complex that mimics a wide complex because of ST depression (the link takes you to such a case). But all other leads confirm that this is wide complex. |
There were no atrial flutter waves uncovered during the pause induced by adenosine, so this is not atrial flutter.
Turns out the patient had asthma, and adenosine can trigger asthma. [An increase in intracellular cAMP in bronchial smoothe muscle cells relaxes them and improves asthma. Adenosine decreases intracellular cyclic AMP; Xanthines such as theophylline increase intracellular cAMP]
She became distressed and SOB, and had a vigorous spasm of coughing, then converted!!
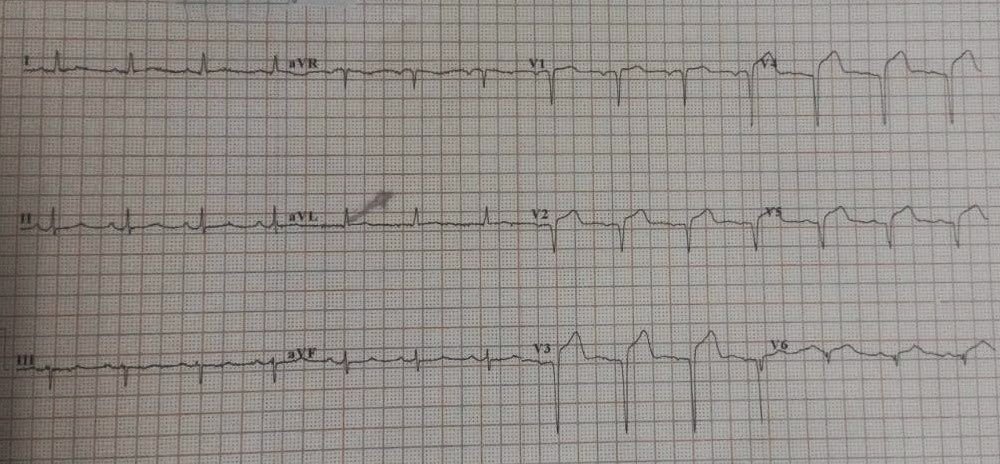
Here is her post conversion ECG:
 |
| Sinus tachycardia at a rate of about 130, with a very short PR interval. Computerized QRS duration is 80 ms. |
Her respiratory distress subsided and she did well.
Analysis
We knew there would be a short PR interval because, by the extremely fast rate of the narrow complex, we knew that the AV node must conduct fast.
What is the diagnosis here? Here is what I wrote to Scott:
–So, there are two abnormalities here:
1) Accelerated AV conduction
2) An accessory pathway (WPW), in which the conduction down the AV node occurs before it can get to the accessory pathway (thus, no delta wave on baseline ECG).
–I believe that the first rhythm was a re-entrant rhythm that went down through that fast AV Node, then up through an accessory pathway (which is equally fast, as they often are).
–After adenosine, the re-entry reversed: it went down through the accessory pathway (Atrioventricular reciprocating tachycardia, or AVRT), with a wide QRS because the accessory pathway activates the ventricle first, and then up through the very fast AV node. See Case 2 of this post for more on AVRT.
–Thus, both rhythms have identical rates, but are going in opposite directions.
–The problem with this explanation is that the beginning of the QRS in both tachycardias is fast. If it were through an accessory pathway, then the beginning of the antidromic rhythm should be wider, and it does not appear to be so.
–The baseline ECG does NOT have any delta wave: the impulse travels down through the AV node too fast for it to make it down the accessory pathway. This is often called “concealed conduction.” See this post for an explanation of Concealed Conduction.–the explanation starts halfway down the page.
–Since the wide complex rhythm has an LBBB configuration, the accessory pathway must be on the right side.
–Alternative explanations:
Dual AV nodal pathways (but why is one tachycardia wide?)
AV nodal pathway with “slow-fast” component (I don’t see how this explains that the latter part of the QRS in the wide complex is slow)
The EP results are back, and:
1. Accelerated AV conduction
2. Left lateral accessary pathway