Written by Pendell Meyers
A woman in her 30s called EMS for acute symptoms including near-syncope, nausea, diaphoresis, and abdominal pain. EMS arrived and found her to appear altered, critically ill, and hypotensive.
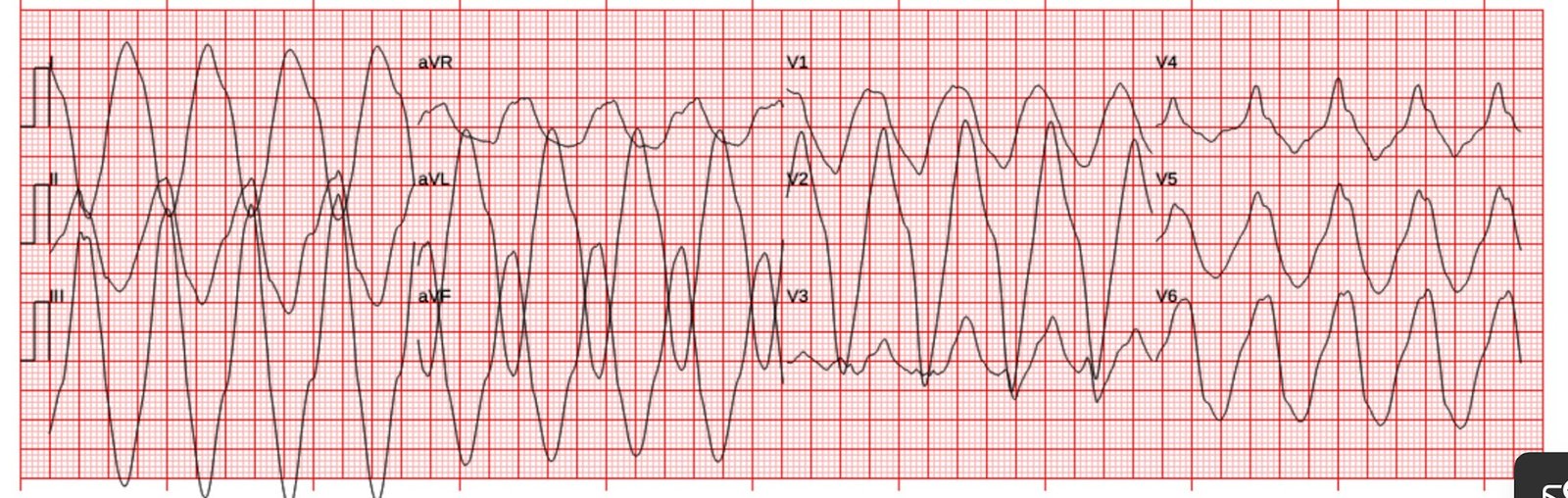
An ECG was performed:
 |
| What do you think? |
Extremely wide complex monomorphic rhythm just over 100 bpm. The QRS is so wide and sinusoidal that the only real possibilities left are hyperkalemia or Na channel blockade. Hyperkalemia is by far more common.
Indeed, further history revealed two missed dialysis sessions. And of course on exam she has a dialysis fistula.
EMS reportedly gave 4 grams of calcium (unknown whether CaCl or gluconate) and 50 mEq of sodium bicarbonate. There was concern that the rhythm might represent ventricular tachycardia, so lidocaine was given and one attempt at cardioversion was performed. It is unclear what changes happened to the rhythm based on the EMS interventions, but the patient arrived to the ED remaining critically ill and with a very wide complex reported (no ECGs from ED available sadly).
Hyperkalemia was diagnosed and more treatment was given including more calcium, bicarb, insulin/dextrose, and albuterol.
The potassium level returned at 9.7 mEq/L.
Emergent dialysis was prioritized after stabilization.
She did well and stabilized after dialysis.
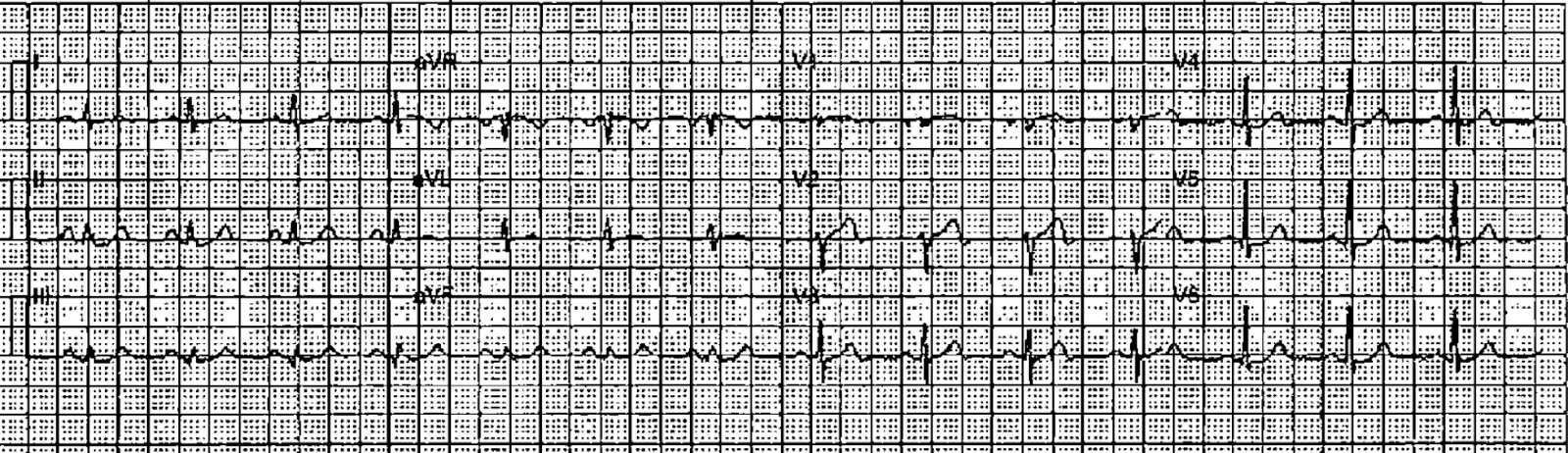
Here is her ECG the next day with normal potassium level:

She did well.
See our other countless hyperkalemia cases below:
General hyperkalemia cases:
A 50s year old man with lightheadedness and bradycardia
Patient with Dyspnea. You are handed a triage ECG interpreted as “normal” by the computer. (Physician also reads it as normal)
Severe shock, obtunded, and a diagnostic prehospital ECG. Also: How did this happen?
A woman with near-syncope, bradycardia, and hypotension
What happens if you do not recognize this ECG instantly?
A woman in her 50s with dyspnea and bradycardia
A patient with cardiac arrest, ROSC, and right bundle branch block (RBBB).
Is this just right bundle branch block?
Is This a Simple Right Bundle Branch Block?
A 60-something who has non-specific generalized malaise and is ill appearing.
HyperKalemia with Cardiac Arrest.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia
What will you do for this altered and bradycardic patient?
I saw this computer “normal” ECG in a stack of ECGs I was reading
What is the diagnosis?
Found comatose with prehospital ECG showing “bigeminal PVCs” and “Tachycardia at a rate of 156”
An elderly woman found down with bradycardia and hypotension
A middle aged man with unwitnessed cardiac arrest
Test almost all of your most important ECG rhythm interpretation skills with this case.
Sinus rhythm with a new wide complex QRS
This ECG is pathognomonic and you must recognize it.
A Very Wide Complex Tachycardia. What is the Rhythm? Use Lewis Leads!!
A Very Wide Complex
Are these peaked T-waves the patient’s baseline T-waves?
Bradycardia, SOB, in a Dialysis Patient
Cases of hyperkalemia mimicking OMI: