A previously completely healthy young man presented to the ED after an episode of palpitations, dizziness and weakness while at work today. He experience a sensation of anxiety and then had sudden onset tightness in his chest, palpitations, dizziness, and weakness. He tried to rest, but his symptoms became worse and he started to sweat profusely. He began to hyperventilate and describes carpal spasm. By the time he arrived in the ED, symptoms were largely resolved. The etiology seemed to be a panic attack, but he had never had one before.
An ECG was recorded:
 |
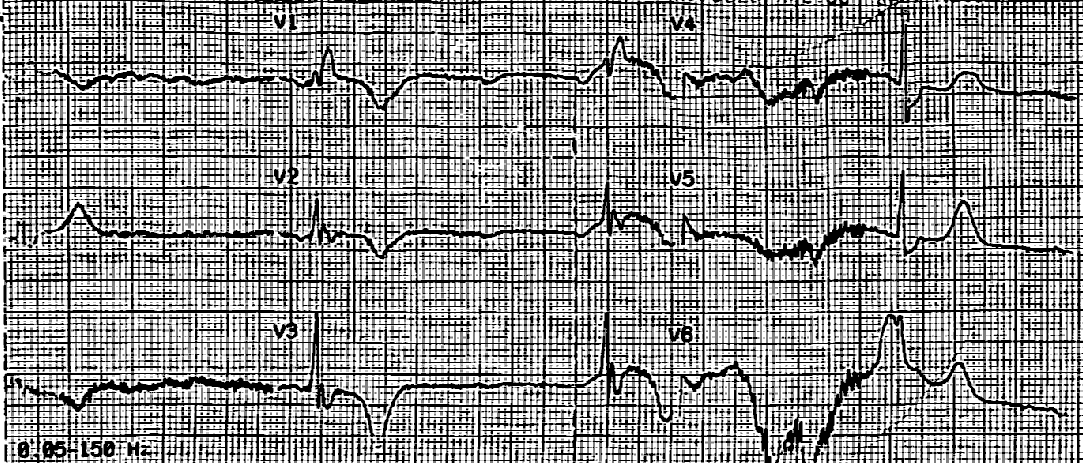
| Besides the RSR’ (right ventricular conduction delay), what do you see? |
There is a long QT (computer measured at 488 ms is correct). There is also a large U-wave fused to the T-wave in V3. Hypokalemia was suspected.
K returned at 2.6 mEq/L.
His K was replenished and he was admitted for monitoring.
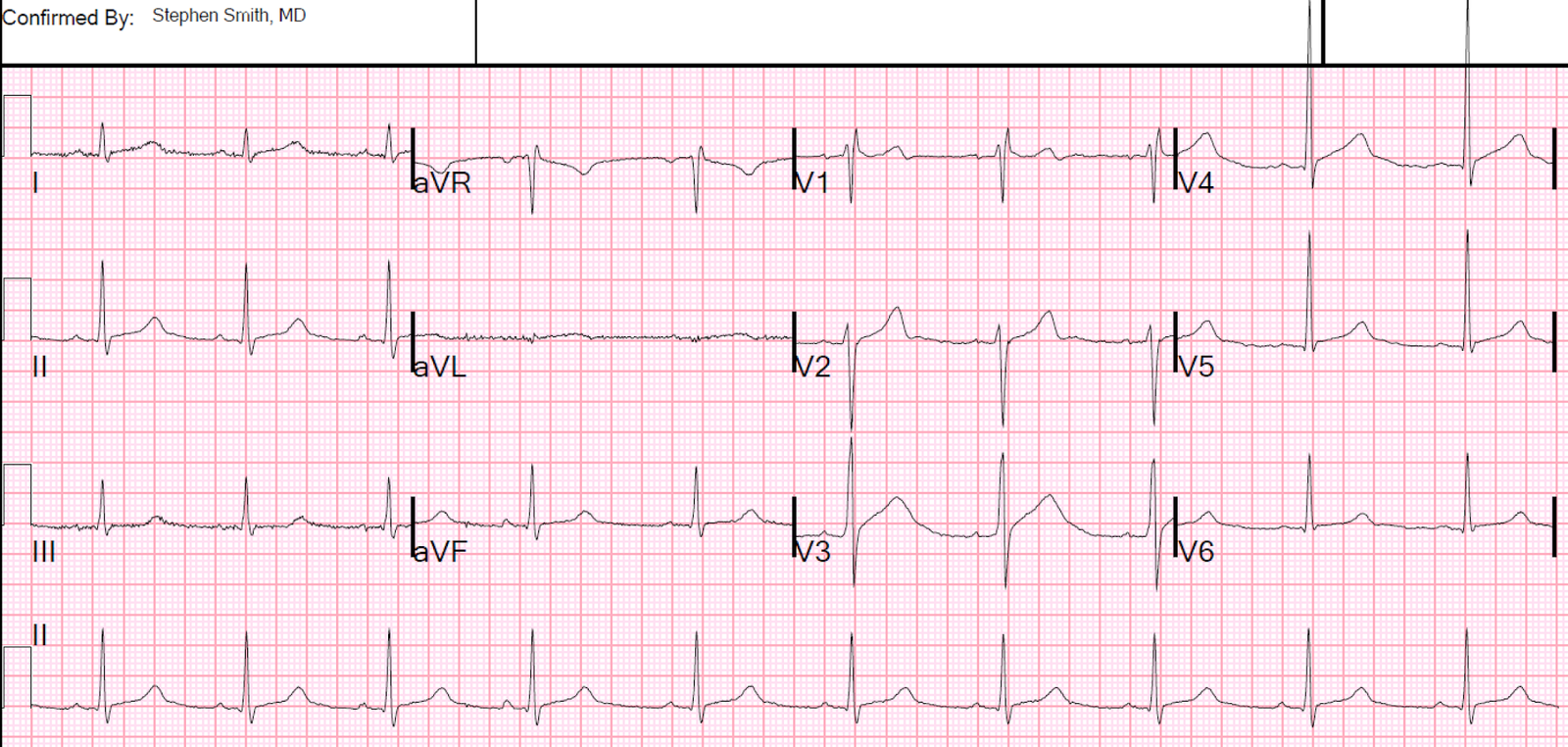
Here is the ECG the next AM with a K of 4.4 mEq/L:
 |
| Normal QT and normal U-waves. RSR’ persists. |
Aside: you might be worrying about type 2 Brugada. It is not type 2 Brugada as the beta angle is too narrow. See this post on Type 2 Brugada Syndrome.
Mg was 1.6 mEq/L. Etiology of hypokalemia would be evaluated as an outpatient. He was discharged.
Discussion
Whether the hypokalemia was the etiology of the symptoms, by causing an unrecorded cardiac dysrhythmia, is uncertain. But severe hypokalemia (K less than 3.0 mEq/L), especially when manifesting on the ECG as ST depression, long QT, or prominent U-waves, is a known cause of cardiac dysrhythmias, including malignant ventricular dysrhythmia.
A low serum K is representative of a VERY low total body K. It cannot be replaced with a single dose of K replacement, as that will immediately redistribute to the intracellular space and hypokalemia will quickly recur. Therefore, severe HypoK requires inpatient replacement with cardiac monitoring.
This ECG shows one of the reasons why it is important to obtain an ECG for syncope or palpitations.
How can you detect severe hypokalemia on the ECG?
Here are several examples. Here are several more interesting cases of hypokalemia.
There is little literature on recognition of hypoK on the ECG. Obvious large U-waves are very specific with a high Positive Predictive Value, but that is not sensitive.
Below is an abstract we wrote back in 2010 in which we identify 3 important variables for diagnosing HypoK. Unfortunately, one is a subjective critierion.
Abstract 400 (ACEP Research Forum): Derivation of a Rule for Diagnosis of Hypokalemia on the Electrocardiogram Get rights and content
Annals of Emergency Medicine, 2010-09-01, Volume 56, Issue 3, Pages S129-S130, Copyright © 2010 American College of Emergency Physicians
There is little data on the electrocardiographic (ECG) diagnosis of hypokalemia (HypoK). We hypothesized the ECG to be an accurate predictor of significant HypoK (K ≤ 2.9 mEq/L) or normoK (K ≥ 3.5 mEq/L) (NormoK).
Study Objectives
Methods
Retrospective study. We searched the electronic medical record for consecutive emergency department diagnoses of HypoK, then hand searched for those in which there was an ECG recorded before administration of potassium (K), and the K was ≤ 2.9 mEq/L. For controls, we searched for consecutive ECGs in patients with K ≥ 3.5 mEq/L. Abnormal QRS (bundle branch block or intraventricular conduction delay) or extreme tachycardia (HR > 130) were excluded, as were redundant patients. One expert reader (ExR) and two resident readers (RRs) who underwent a short tutorial interpreted the randomly sorted ECGs while blinded to the K level and the Bazett-corrected QT interval (QTc-B). ECGs were analyzed for computerized QTc-B, presence of U-waves [None (NUW), subtle (SUW), or prominent (PUW)], T-Wave flattening (TF), and ST segment depression (STD). Resident readers combined, and the expert reader, noted subjective interpretations (SI, either ExR-SI or RR-SI) [definite HypoK (SI+), or not]. Analysis was by descriptive statistics, by Student’s t-test and by Chi-square (CS).
Results
There were 100 cases of HypoK with an ECG; 13 were excluded, leaving 87. There were 58 controls. QTc-B was the single best differentiator, with accuracy (Acc) of 74%. Expert reader Acc was 72%, and Resident reader was 63% (p=.10 by CS). Mean QTc-B for HypoK was 475 ± 8.2 milliseconds (ms); for NormoK is was 429 ± 5.5 ms (p<0 .0001="" 100="" 3="" 78="" 79="" 80="" 83="" 86="" 89="" 92="" 98="" a="" acc.="" acc="" added="" and="" best="" by="" combination="" criteria="" diagnosis="" exr="" font="" had="" if="" none="" objective="" of="" or="" prolonged="" prominent="" qtc-b="" results="" rrs="" s="" sens="" spec="" student="" subjective="" t-test="" the="" these="" to="" two="" u-wave="" versus="" was="" were="" with="">
Conclusion
QTc is longer in HypoK than NormoK. Significant HypoK in the ED can be recognized on the ECG with high accuracy using QTc-B and presence of prominent U-waves. HypoK can be recognized with very high Sens, Spec, and Acc, using subjective interpretation of either the expert reader or the residents, plus QTc-B and presence or absence of prominent U-waves.