A 78 yo male had a syncopal event and complained of chest pain.
Here are 9 prehospital ECGs during transport:
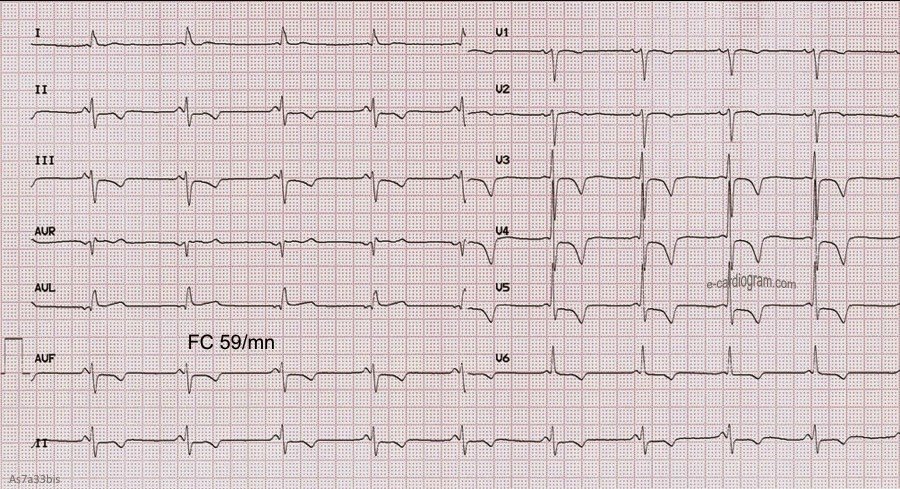
 |
| 0 minutes, nondiagnostic |
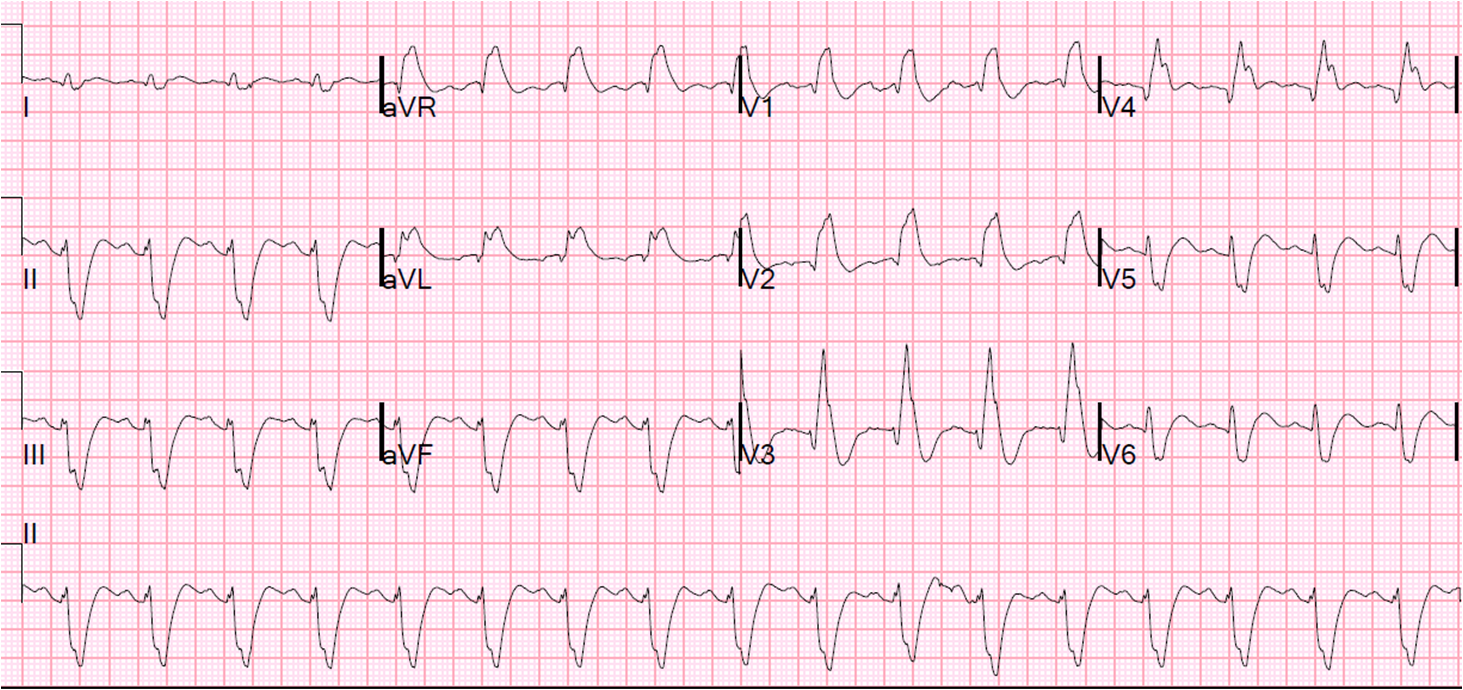
 |
| 4 minutes, inferior STEMI (subtle). |
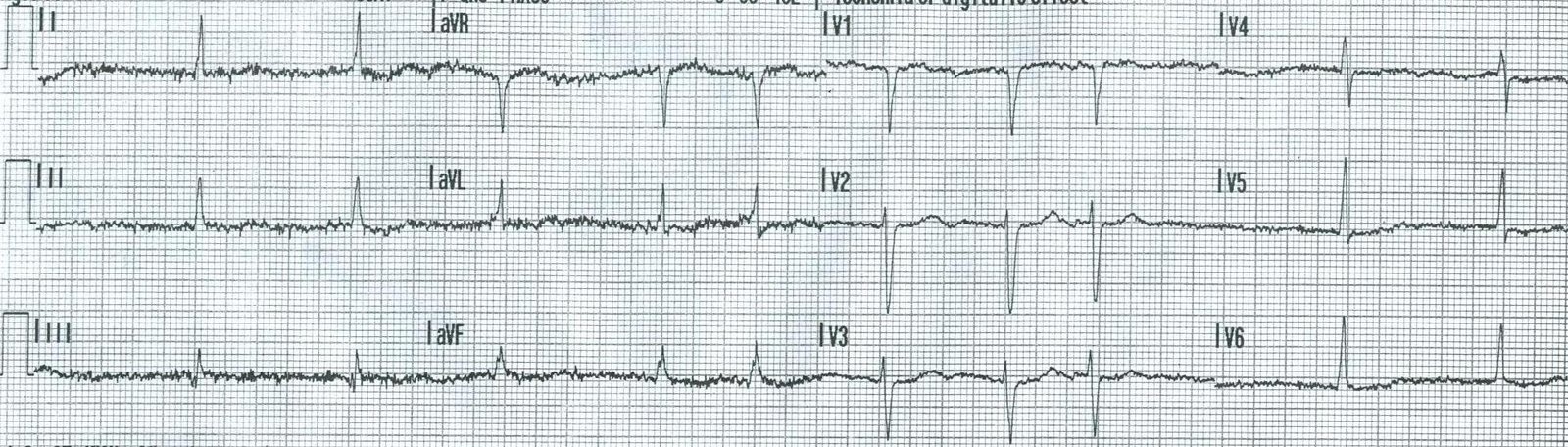
 |
| 5 minutes, reperfused, barely shows on the ECG |
 |
| 7 minutes, almost normal again. |
 |
| 15 minutes, more obvious |
 |
| 16 minutes, more obvious, NTG given here |
 |
| 22 min, with V4R, STE gone after NTG and Aspirin |
 |
| 23 minutes, very subtle, resolving |
 |
| 29 minutes, almost entirely resolved |
The cath lab was activated prehospital and the patient received an RCA stent and an LAD stent, had a minimal troponin rise, and did well.
This shows how acute coronary syndrome is very dynamic, with arteries opening and closing. Studies using continuous 12-lead monitoring show that this happens even in the abscence of chest pain.