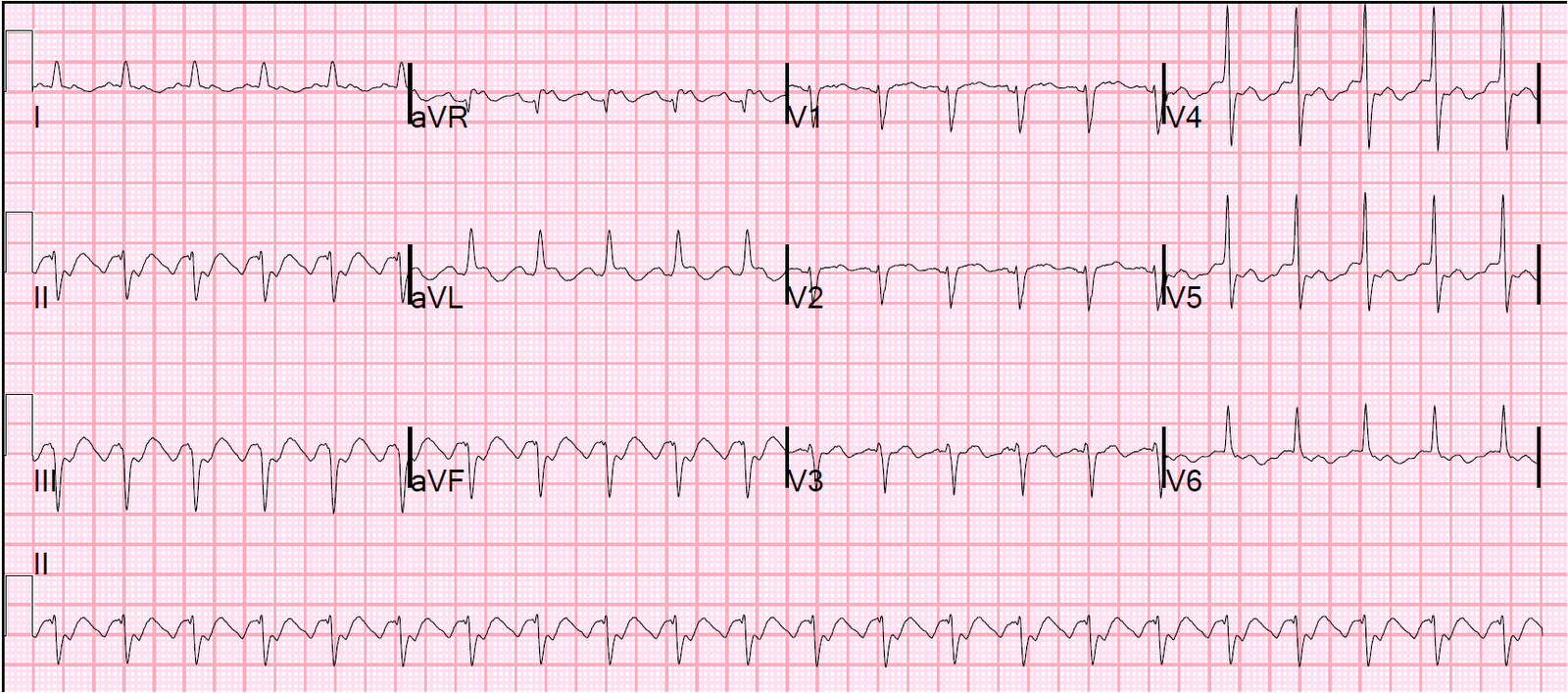
A 52 year old male presented with epigastric pain, continuing in the emergency department. He has a history of hypertension, and is on amlodipine. Thinking that epigastric pain might be an anginal equivalent, this ECG was recorded:
 |
|
|
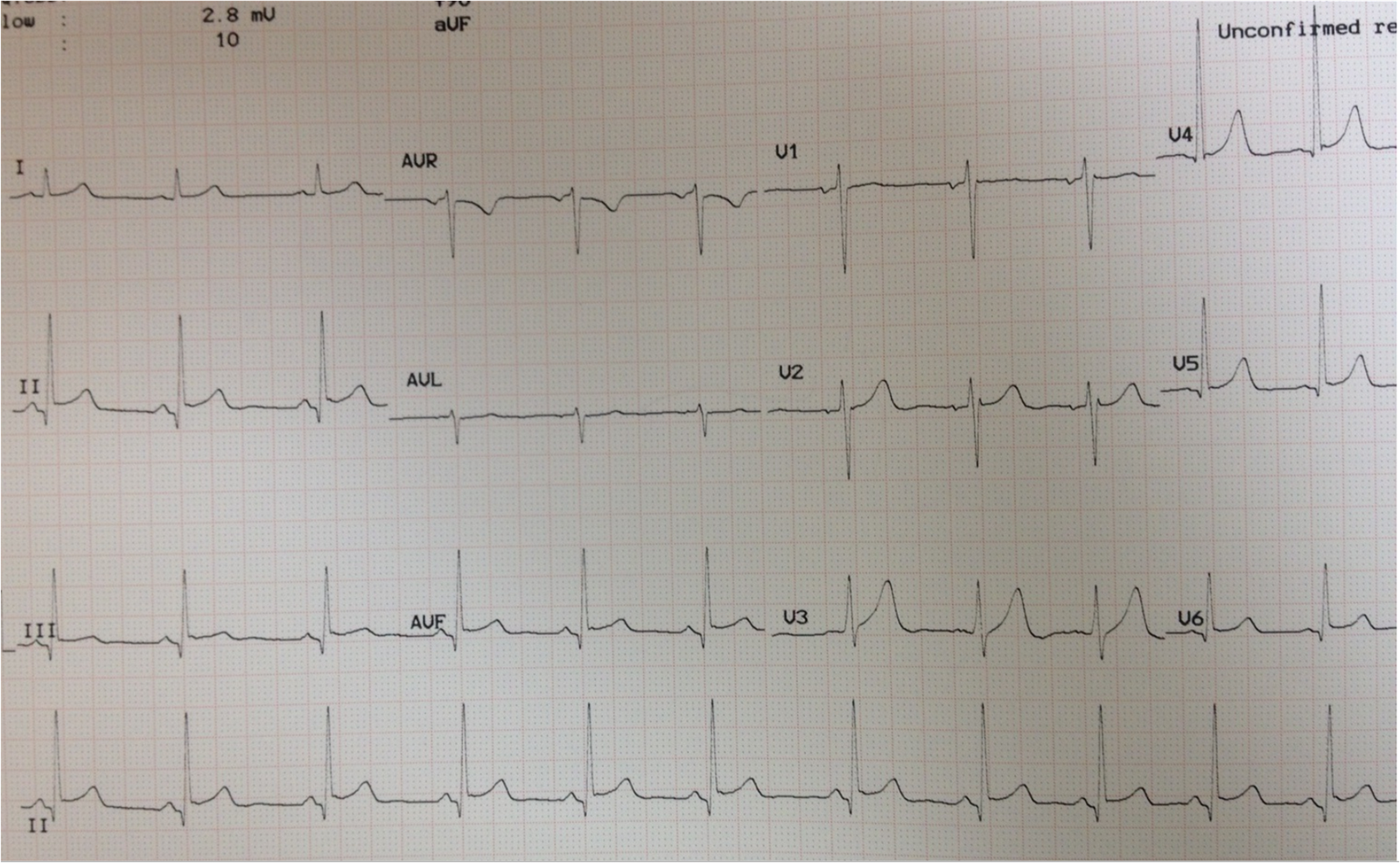
The physicians were worried about Wellens’ syndrome and treated for ACS. He was placed on a nitroglycerine drip. Initial troponin was negative. A followup ECG was done 3 hours later.
 |
|
|
He was admitted. All troponins were normal. A formal echo showed concentric LVH and there was also a subtle abnormality which the echocardiographer thought suspicious for LAD distribution ischemia. So he underwent a coronary angiogram which was completely normal.
This is not Wellens’. Why?
1. LVH frequently causes T-wave inversion which mimics Wellens’
2. In Wellens’, the chest pain is nearly always resolved by the time of the ECG. It is reperfusion that results in the T-wave inversion and the pain is thus resolved by this time.
3. Wellens’ is defined by chest pain and ECG abnormalities. Though Acute MI can present as epigastric pain, it is not at all common and T-wave inversion in the setting of epigastric pain is not high risk for ACS.
4. T-wave inversion in Wellens’ is primarily V2-V4. When T-wave inversion is V3-V6, one should think more about LVH or Benign T-wave Inversion (this post on Benign T-wave Inversion is worth reading)