Benign T-wave Inversion from HQMedEd on Vimeo.
There are many etiologies of T-wave inversion. We are most worried about ischemic T-wave inversion. Wellens’ syndrome is particularly dangerous, as it signifies an unstable critical LAD stenosis. I have several posts on this; here is one that shows the entire evolution.
Another etiology is “Benign T-wave Inversion”, which has long been recognized. I first saw it described in Chou’s textbook. It is a normal variant associated with early repolarization. K. Wang recently studied it. He reviewed ECGs from all 11,424 patients who had at least one recorded during 2007 at Hennepin County Medical Center (where I work) and set aside the 101 cases of benign T-wave inversion. 97 were black. 3.7% of black men and 1% of black women had this finding. 1 of 5099 white patients had it. Aside from an 8.8% incidence (9 of 109) black males aged 17-19, it was evenly distributed by age group.
I have reviewed these 101 ECGs, and what strikes me is:
1. There is a relatively short QT interval (QTc < 425ms)
2. The leads with T-wave inversion often have very distinct J-waves.
3. The T-wave inversion is usually in leads V3-V6 (in contrast to Wellens’ syndrome, in which they are V2-V4)
4. The T-wave inversion does not evolve and is generally stable over time (in contrast to Wellens’, which evolves).
5. The leads with T-wave inversion (left precordial) usually have some ST elevation
6. Right precordial leads often have ST elevation typical of classic early repolarization
7. The T-wave inversion in leads V4-V6 is preceded by minimal S-waves
8. The T-wave inversion in leads V4-V6 is preceded by high R-wave amplitude
9. II, III, and aVF also frequently have T-wave inversion.
Below are 5 examples, followed by a case of Wellens.’
I show you the LAD-BER formula calculations, but remember, strictly speaking, this was not studied in ECGs with: 1) T-wave inversion, 2) coved (upwardly convex) ST segments, or 3) LVH.
Here is the formula; there is an excel spreadsheet down the right side of this blog: (1.196 x STE at 60 ms after the J-point in V3 in mm) + (0.059 x computerized QTc) – (0.326 x R-wave Amplitude in V4 in mm). A value greater than 23.4 is quite sensitive and specific for LAD occlusion.
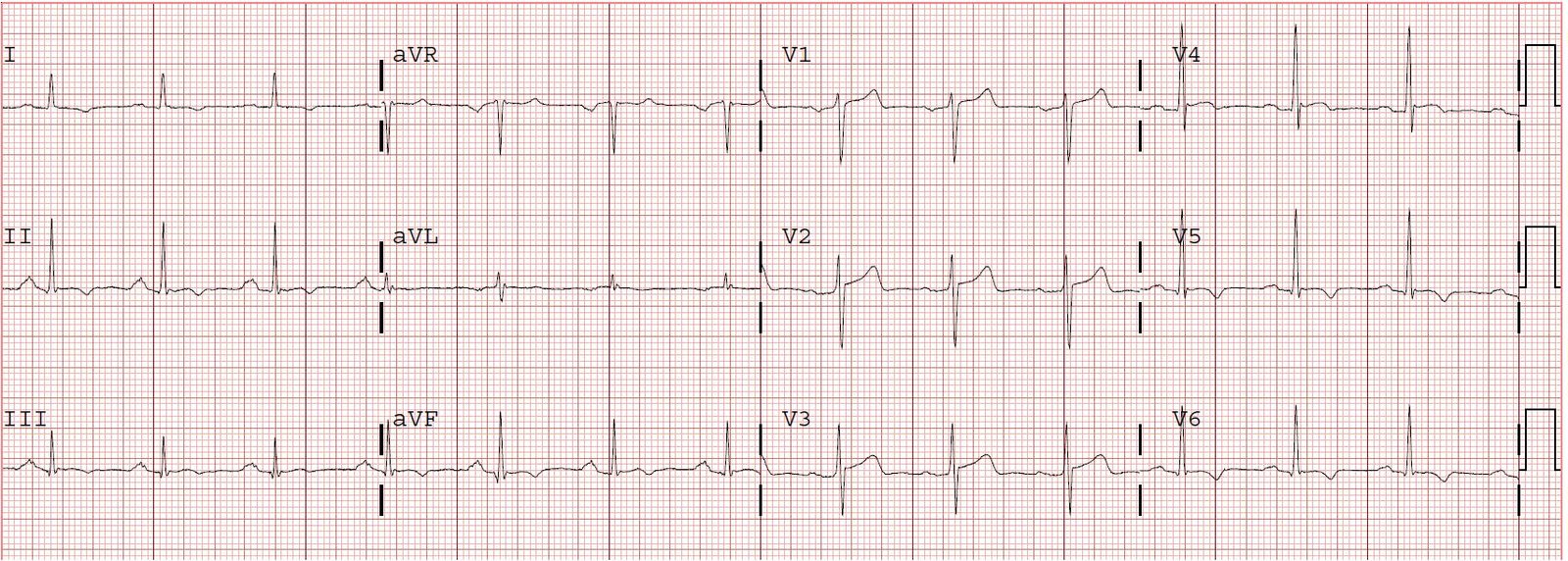 |
| Benign T-wave inversion: There is ST elevation in V2 and V3, with T-wave inversion in left precordial leads. QTc = 395ms, formula value (to determine if the STE is STEMI or not) = 21.13 (< 23.4 is early repol). Note the prominent J-waves, the minimal S-waves and the prominent R amplitude in leads with T-wave inversion. |
 |
| Benign T-wave Inversion: This has some scary looking STE and TWI. QTc is 415ms and formula value is 21.39. |
 |
| Benign t-wave inversion. QTc = 415, formula = 18.5 |
 |
| Benign T-wave inversion and probable LVH. Scary ST elevation, right? But QTc is 421ms and formula value is 20.17. |
 |
| Benign T-wave Inversion? QTc 398, formula 17.6. This one was not stable. The next day it was gone. It was recorded in a young black male with chest pain. There were negative serial troponins but no angiogram. Dr. Wang considered it to be BTWI. |
 |
| Wellens’ syndrome. Note the evolution from A to C. It begins with terminal T-wave inversion (biphasic) in lead V2, later extends to V3 and V4, and still later becomes deep and symmetric and only then extends to V6. There was a critical LAD stenosis. In this case I do not know what the computerized QTc was. This is taken from an article I wrote in EM Clinics of North America 2006;24(1):53-89. |