This is courtesy of Mohammed S. Alo, who kindly let me reproduce a case from his blog (Mohammed Alo’s blog).
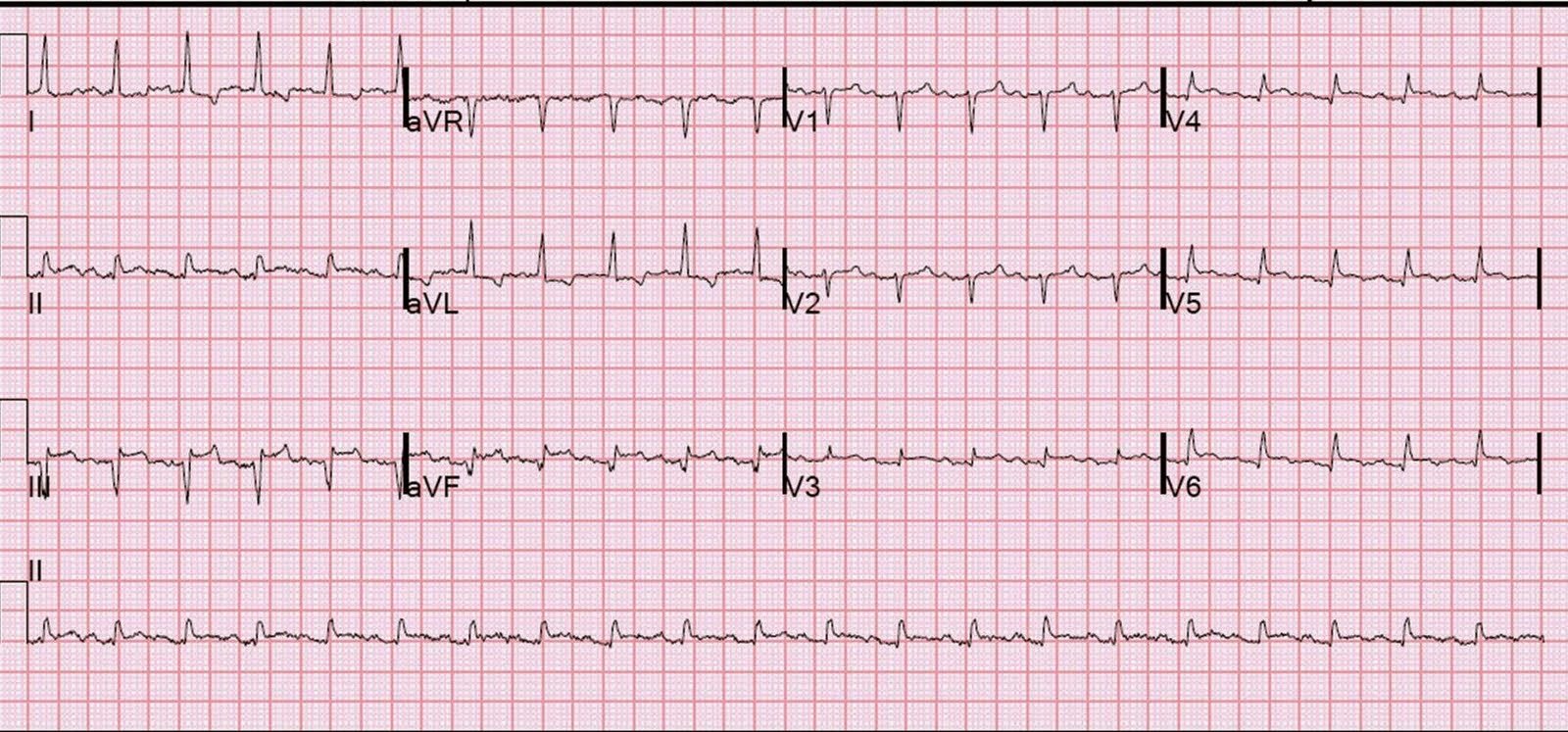
This is a 40 year old male with chest pain. The cardiologist was called for management of a STEMI:
 |
| It is sinus rhythm, and there is slightly wide and abnormal appearing QRS, with an rSR’ (though I don’t think the duration is long enough to be RBBB, but that is a bit hard to read). There is significant ST elevation in V2 and some in V3. There is “saddleback” ST elevation. However, it just does not have the appearance of anterior STEMI. |
First, when assessing any ST-T abnormalities, one must determine if they are “primary” (due to pathology such as ischemia or hypokalemia, etc.) or “secondary” to an abnormal QRS. And here the QRS is abnormal. Then, think if it conforms to any known pathologic morphology. If you do, and you are aware of the 3 forms of Brugada syndrome, you will see that this is very similar to Type II Brugada.
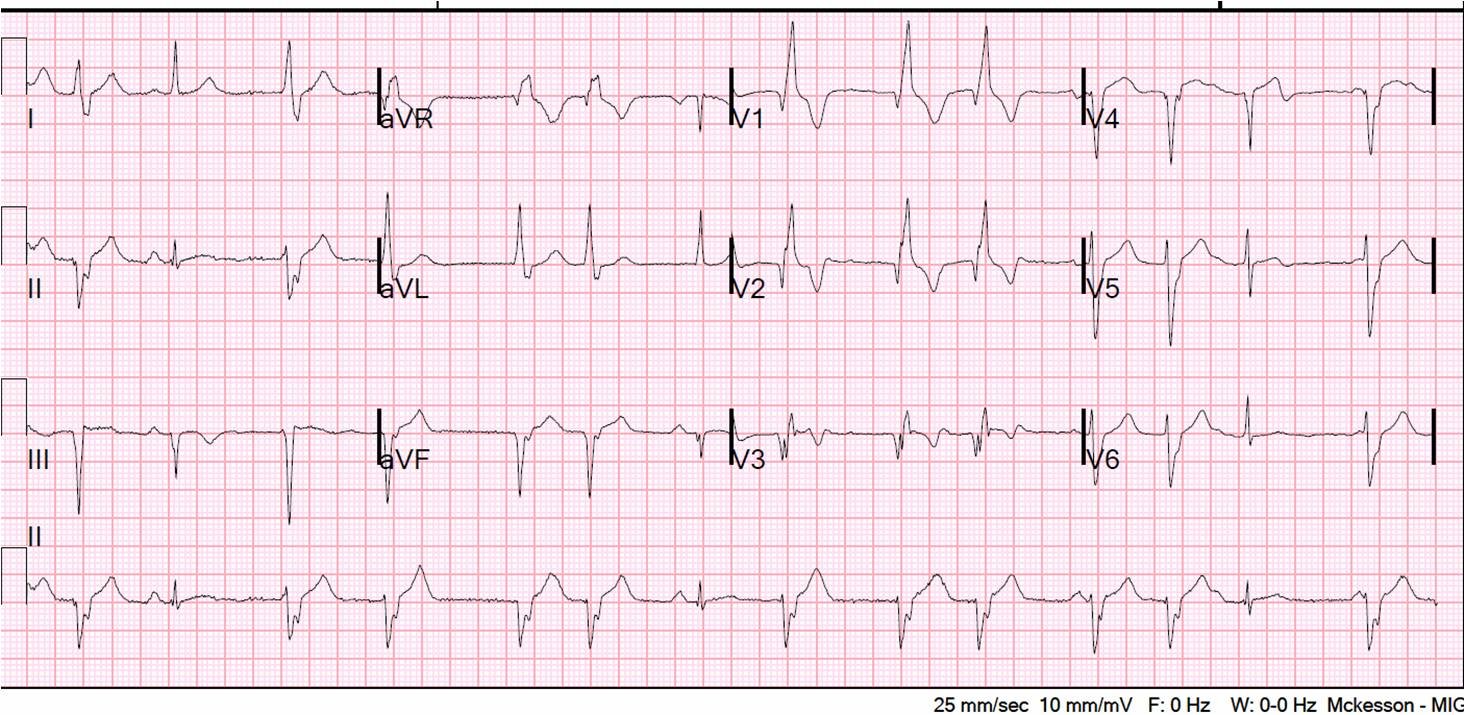
Here is another case with “saddleback” ST elevation.
Here are the 3 types:
Type I: (“Coved type”) V1 has an incomplete RBBB, a wide R’ wave, a downsloping ST segment, and in inverted T-wave, like this:

Types II and III) These have a saddle back ST-T wave, as in the case presented. The ST segment is at least 1 mm in Type II and less than 1 mm in Type III
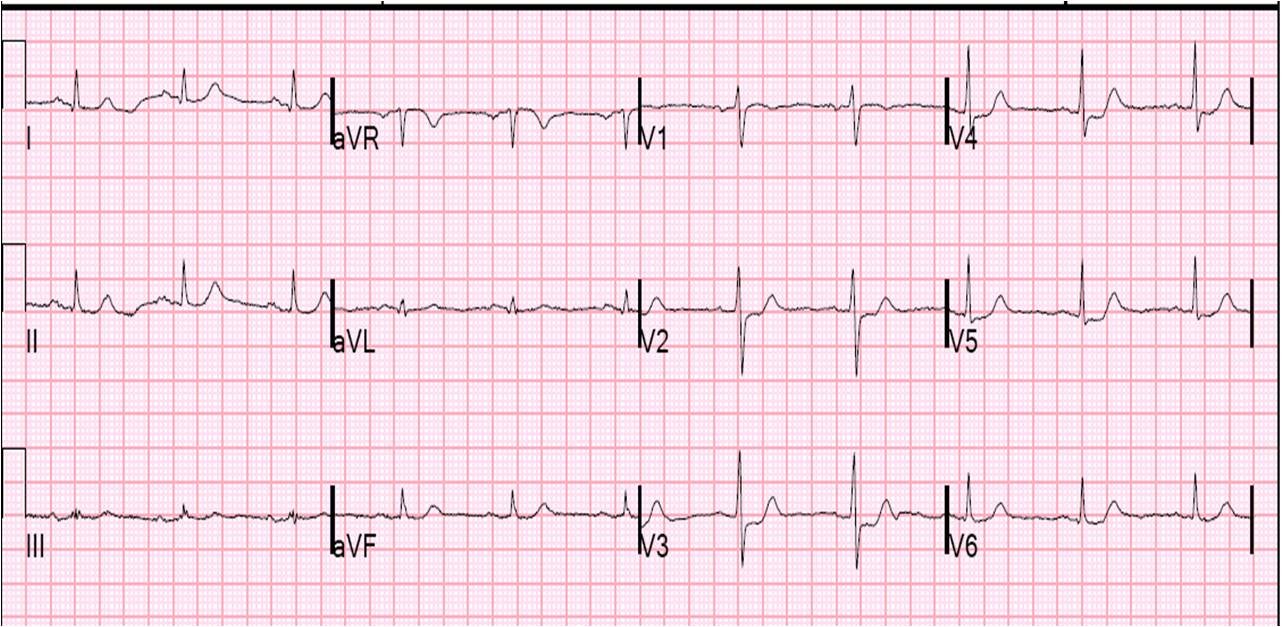
There are also variants of early repolarization that can mimic Brugada. Here is one that mimics type III Brugada (again, sorry it cannot be enlarged):

Case conclusion: the man did indeed have Type II Brugada ECG, not Anterior MI.
Brugada pattern ECG does not necessarily mean the patient has Brugada syndrome. Here are the 2002 consensus diagnostic criteria for Brugada syndrome.
Type I Brugada
Appearance of type 1 Brugada pattern in more than one right precordial lead (V1-V3) in the presence or absence of a sodium channel blocker, and at least one of the following:
1) Documented ventricular fibrillation
2) self-terminating polymorphic ventricular tachycardia (VT)
3) Family history of sudden cardiac death at <45 years
4) Type 1 ST segment elevation in family members
5) Electrophysiologic inducibility of VT
6) Unexplained syncope suggestive of a tachyarrhythmia
7) Nocturnal agonal respiration
Type 2 and type 3 Brugada syndrome — a type 2 or type 3 Brugada ECG who meet both of the following criteria [7]:
1) Appearance of type 2 or type 3 ST segment elevation (saddle-back type) in more than one right precordial lead under baseline conditions, with conversion to type 1 following challenge with a sodium channel blocker.
2) One of (a-g) above.
•Appearance of type 1 ST segment elevation (coved type) (figure 2) in more than one right precordial lead (V1 – V3) in the presence or absence of a sodium channel blocker, plus at least one of the following:
a) Documented ventricular fibrillation
b) Self-terminating polymorphic ventricular tachycardia (VT)
c) Family history of sudden cardiac death at <45 years
d) Type 1 ST segment elevation in family members
e) Electrophysiologic inducibility of VT
f) Unexplained syncope suggestive of a tachyarrhythmia
g) Nocturnal agonal respiration