Published study: When the ECG was very difficult, the Queen was 7.36 times more likely to be correct than the Standard of Care.
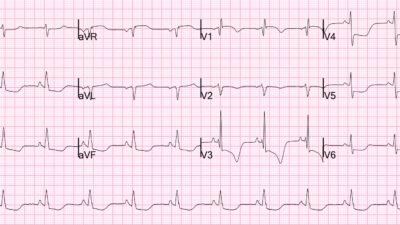
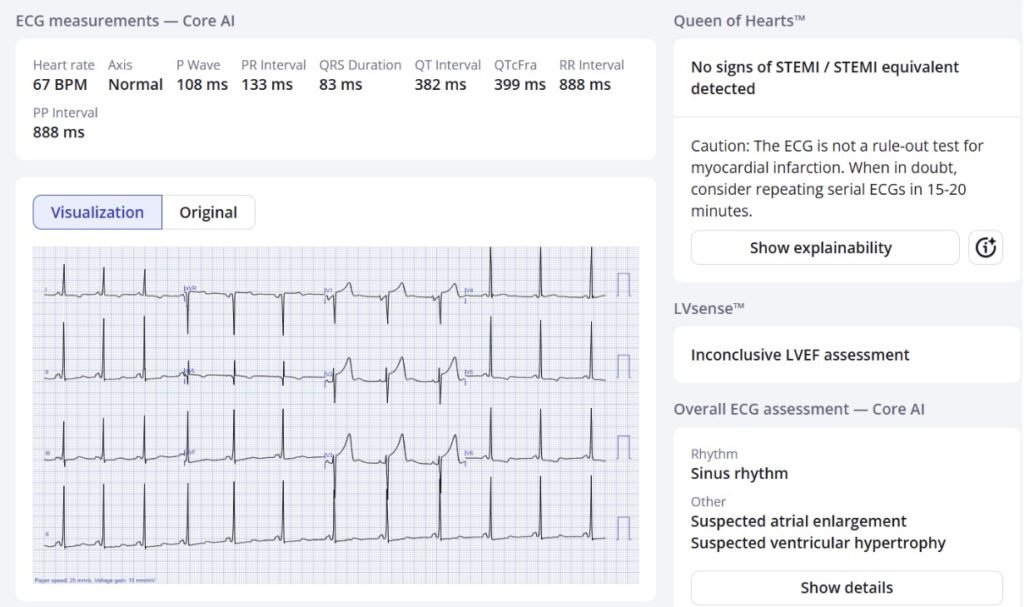
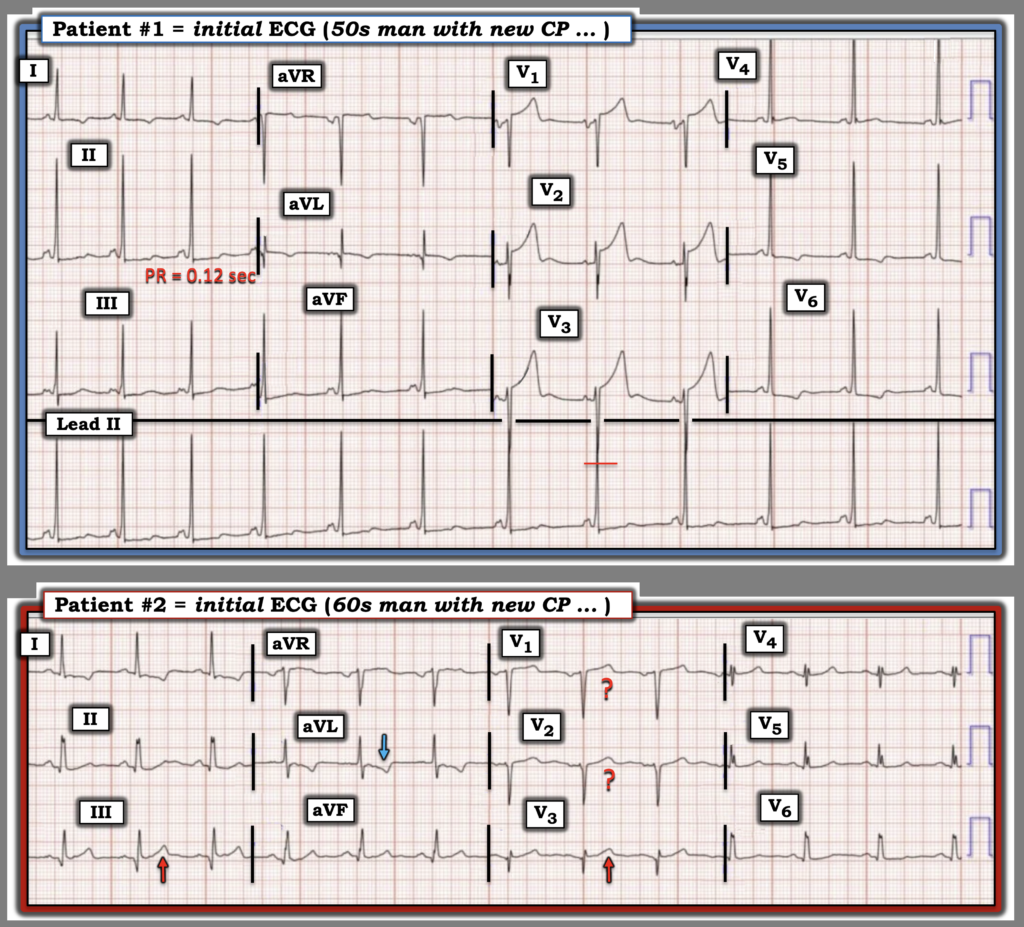
Patient #1: Man in his 50s with acute atraumatic chest pain, normal vital signs, and this triage ECG:
What do you think?
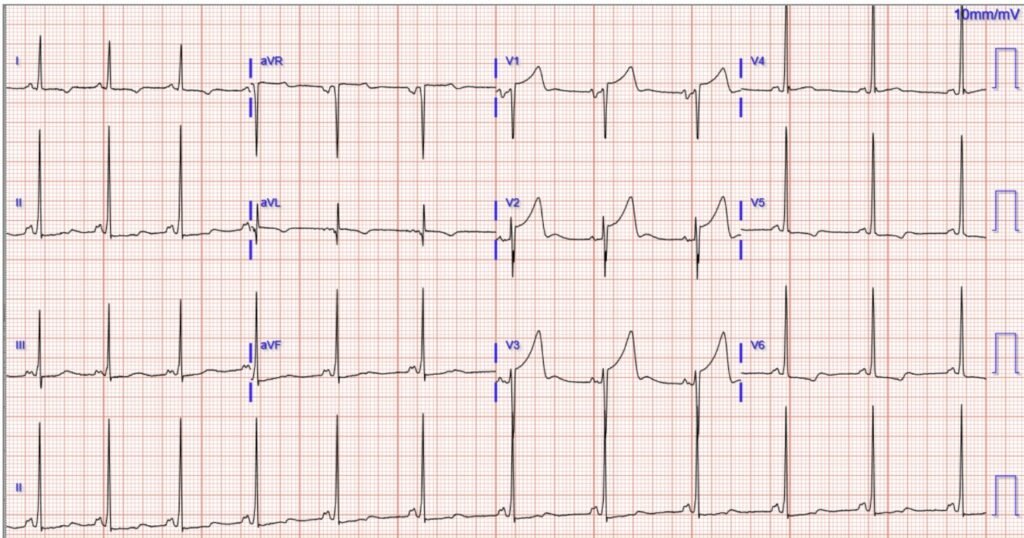
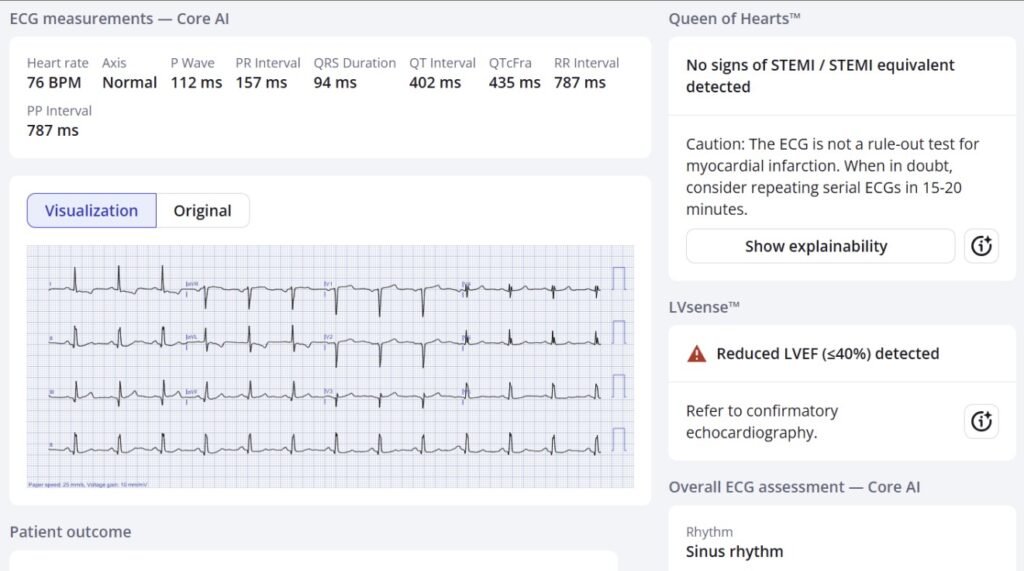
Patient #2: Man in his 60s with acute atraumatic chest pain, normal vital signs, and this triage ECG:
What do you think?
Which patient, both, or neither have ECG signs of acute coronary occlusion and need emergent reperfusion?
Here’s what the Queen of Hearts thinks:
Patient 1:
Patient 2:
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical). As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: PMcardio is CE-certified for marketing in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA.
Smith: I looked at them both without any information and immediately could tell that they are both mimics (“Not OMI”, or “No signs of STEMI/STEMI Equivalent”).
Pendell continues:
Both patients were suspected to be “STEMI” by the treating physician. The cath lab was activated overnight for both of them, and they both had normal coronary angiograms and serial negative troponins.
No other dangerous cause of symptoms was discovered and both were discharged in good condition.
Both ECGs are mimics of ischemic ST elevation. See Ken Grauer’s detailed analysis below. Case 1 is LVH mimicking precordial swirl. Case 2 is a type of baseline variant that I do not have a particular name for, but have seen many times. Case 2 may also have LVH features causing the downsloping STD/TWI in high lateral leads.
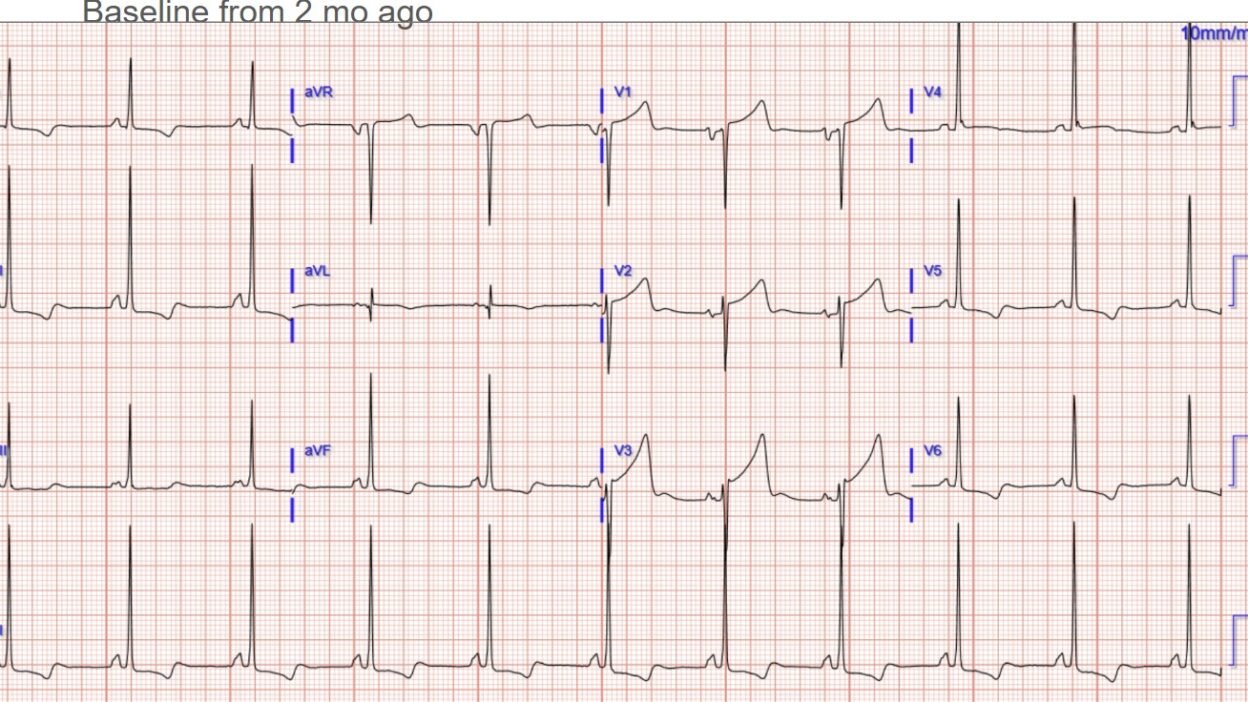
Patient 1 had a baseline ECG available, but it was found only after the cath lab:
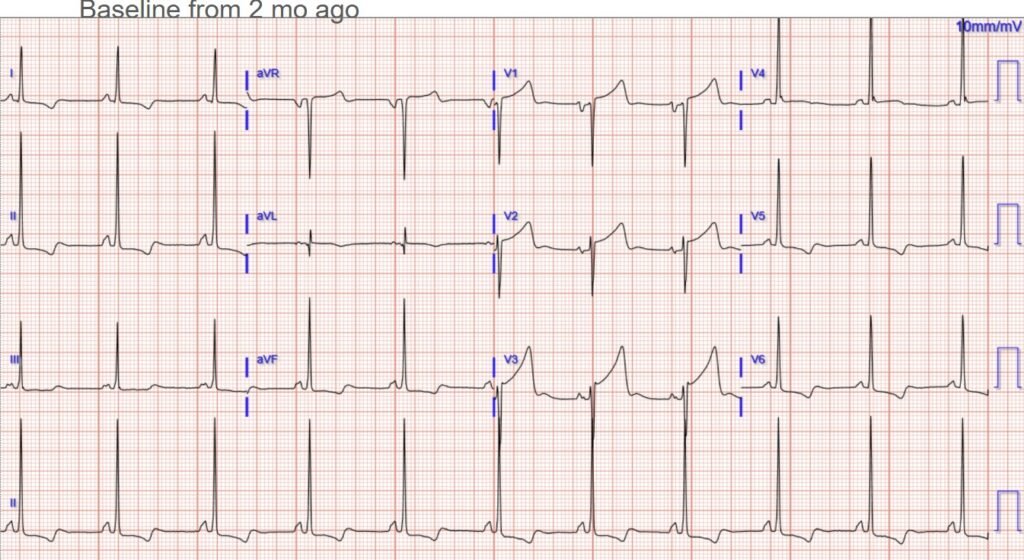
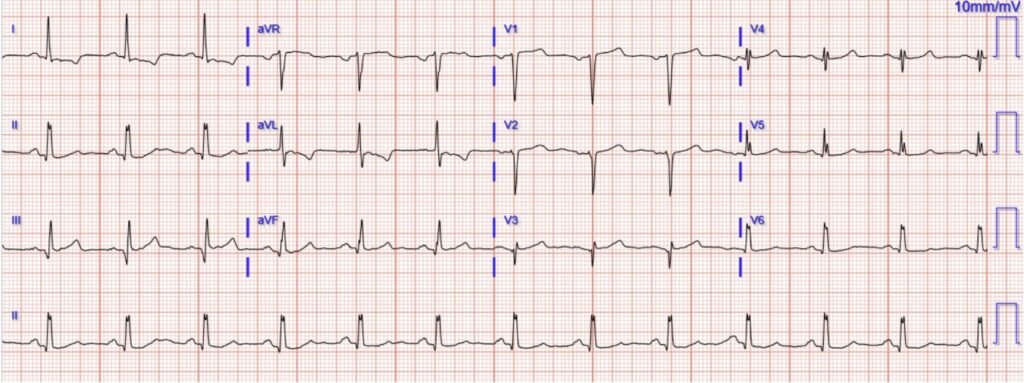
Patient 2 had no baseline available.
False positive cath lab activation due to difficult ECGs is a common and important problem, even if it is not as important as the many missed OMIs on the other side of the coin. Both can be greatly improved upon by developing (or using) ECG expertise.
We here at Dr. Smiths ECG Blog have been trying our hardest since ~2008 to help everyone learn it for free! And we always will be free here on the blog. For those who also want to utilize AI for this purpose, we are trying our best to make the Queen as accurate as possible.
Smith: Now and then, I get ECGs sent to me that are false positives by the Queen, or False negatives. Everyone should realize that the Queen is not perfect. We are constantly making her better, but she is not perfect. However, humans are much less perfect. There are those who criticize self-driving cars because occasionally there is a motor vehicle accident due to AI driving; but humans are much worse.
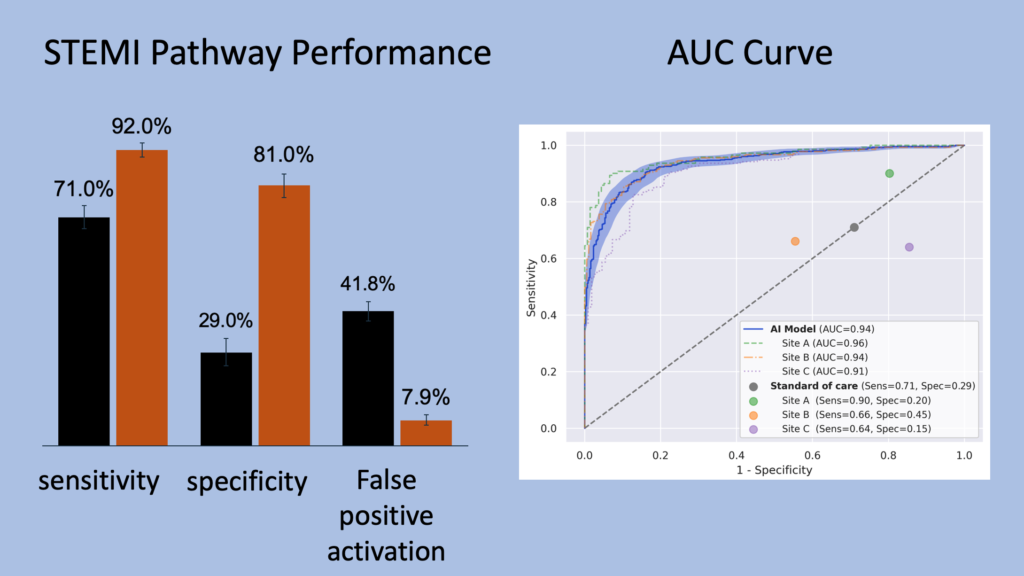
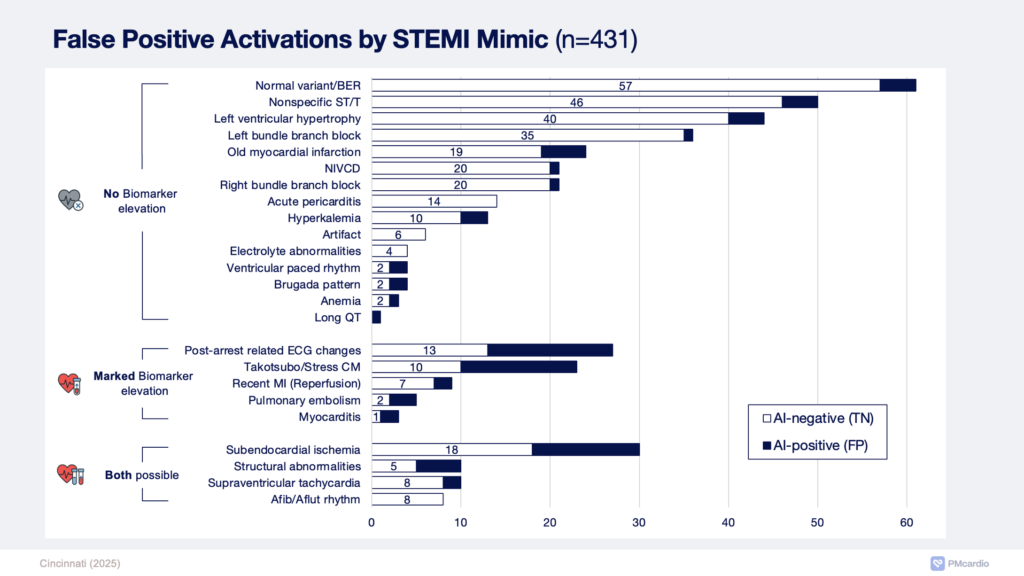
—–We published a recent study comparing Queen to Standard of Care Cath lab activations (and remember that “standard of care” is the physicians with the ECG, symptoms, records, old ECG, bedside echo, etc.). The Queen has no context to help her; all she has is the ECG itself. The physician or medic must use the context to interpret her result. The Queen decreased false positives from 42% to 8% while increasing sensitivity on the first ECG from 71% to 92%. The Queen did have some false negative and positives. But this table below shows us that sometimes the ECG is very hard (75 ECGs in which both Queen and Standard of Care were wrong), and sometimes it is easy (497 cases in which both were correct). But in the difficult cases, in which either Queen or Standard of Care was wrong, the Queen was correct in 405 cases, whereas the Standard was correct in 55 cases.
When the ECG was very difficult (ECG and standard discordant), the Queen was 7.36 times more likely to be correct than the “Standard of Care”.

= = =
======================================
MY Comment, by KEN GRAUER, MD (3/13/2026):
The important question that is posed in today’s challenging post by Dr. Meyers is — Whether the 2 patients with acute CP in today’s case need emergent reperfusion on the basis of their initial ECG?
- I find cases like these to be especially insightful — because we have the cath results that tell us the Answer.
- That said — I’ll offer a slighty different approach to this challenge.
= = =
My Approach:
The moderation I add to my approach, is that instead of restriction to 2 Answers (ie, That emergent cath with PCI is or is not immediately needed) — I favor consideration of a 3rd possible Answer — which in today’s post was that I was not yet ready to render a definite answer for Patient #2 on the sole basis of his triage ECG.
- Obviously — We can not delay a lot. “Time is Muscle (myocardium)”. As emphasized by Drs. Smith and Meyers in the February 8, 2026 post — the October 23, 2025 post — the January 15, 2026 post, and many others — the most benefit from reperfusion occurs within the first 4 hours after acute coronary occlusion (Every 2-hour delay results in 60% more myocardium infarcted).
- The above said — in most cases it should be possible to decide on the need for prompt cath within minimal time pending some additional information, to include: i) One or more repeat ECGs (with the 1st repeat tracing done within the next 10-15 minutes); — ii) A bit more history (with ongoing follow-up on how the patient is doing); — iii) At least the initial Troponin result (realizing that a 1st Troponin that is normal does not completely rule out an acute event); — and, iv) Assessment by bedside Echo recorded during CP, looking for a localized wall motion abnormality (which if found would support the need for immediate catheterization).
= = =
Regarding the Initial ECG from Patient #1:
I would not activate the cath lab on the basis of Patient #1‘s initial ECG — as I felt this tracing was most suggestive of LVH with “strain”. As shown in Figure-1:
- QRS amplitude is markedly increased in multiple leads — satisfying many of the Voltage Criteria most commonly cited for LVH (ie, Inferior lead R waves >>20 mm — deep S wave in lead V3 [that overlaps with the tall R wave in the long lead II rhythm strip] — very tall R wave in lead V4 that is truncated by the limits of the ECG paper — R wave ≥25 mm in lead V5 — R wave >18 mm in lead V6).
- ST-T appearance is typical for LV “strain” in multiple left-sided leads (= leads I,V5,V6 — each of which show slowly downsloping ST depression that finishes with a more rapid terminal return of the T wave to baseline).
Other features to note regarding Patient #1‘s initial ECG:
- Although there is considerable J-point ST elevation in leads V1,V2,V3 — as discussed in My Comment in the June 20, 2020 post — LV “strain” in some patients with LVH may be seen in anterior leads, which manifest the mirror-image opposite picture of LV “strain” that we are used to seeing in left-sided leads (ie, concave upward-sloping ST segments with J-point elevation in leads V1,V2 and/or V3).
- NOTE: The PR interval looks “short” (I measure it at the lower normal limit for sinus conduction in an adult = 0.12 second). In addition — several leads seem to show slight distortion of the initial R wave upslope. To Emphasize: I would not diagnose WPW in this patient — as we do not see clear sign of delta waves. But the PR interval in this tracing is uncharacteristically short for a 50-year old — and AP (Accessory Pathway) conduction can be both intermittent and partial — such that it would be prudent to get more history and review additional tracings on this patient to ensure that we are not seeing partial preexcitation.
- Bottom Line: I strongly suspected an LVH “fake” as soon as I saw this tracing. As a result — I would not activate the cath lab based on this initial ECG from Patient #1. That said — the relative amount of J-point ST elevation in leads V1,V2 in this patient who presented to the ED for acute CP is more than what I’d typically expect for anterior lead LV “strain”. I’d therefore repeat the ECG and obtain serial Troponins to confirm my impression that this is an LVH “fake”.
= = =
Figure-1: Comparison between the 2 initial ECGs in today’s case.
= = =
The Initial ECG from Patient #2:
I interpreted the initial ECG from Patient #2 as non-diagnostic. As a result — I would not activate the cath lab on the basis of this initial tracing. That said — I thought there were some atypical features that in this 60s man who presented to the ED for acute CP merited confirmation that nothing acute was ongoing.
- The rhythm is sinus at ~75/minute. Intervals and the axis are normal — and there is no chamber enlargement.
- The inferior lead q waves are small and narrow, and probably insignificant. Tiny normal septal q waves are seen in lateral leads I,V5,V6.
- R wave progression — is remarkable for tiny initial r waves in leads V1,V2, and suggestion of an initial Q wave in lead V3.
- T wave appearance caught my “eye” in a number of leads: i) The T wave in lead V3 (in which there appears to be an initial Q wave) — looks disproportionate to the tiny r wave in this lead, especially given slight ST elevation in lead V3; — ii) The ST-T waves in leads V1,V2 would look consistent with anterior LV “strain” — except that no leads on this tracing come close to satisfying LVH voltage criteria; — and, iii) The upright T wave in lead III — and the negative T wave in lead aVL both look more peaked than I’d normally expect, especially given modest QRS amplitude in these leads.
- To Emphasize: I did not think any of these changes were diagnostic of an acute event — and I would not have activated the cath lab on the basis of this initial ECG. But given that this 60s man presented to the ED because of acute CP — I would want to repeat the ECG — check serial Troponins — and do a bedside Echo to confirm my impression that Patient #2 was not having an acute event.
= = =
= = =