I’m reposting an edited version of this post from June 2009.
This is a 46 yo male with acute onset of chest pain, in distress, who
called the ambulance. He arrived and had this ECG recorded at 0118 AM.
 |
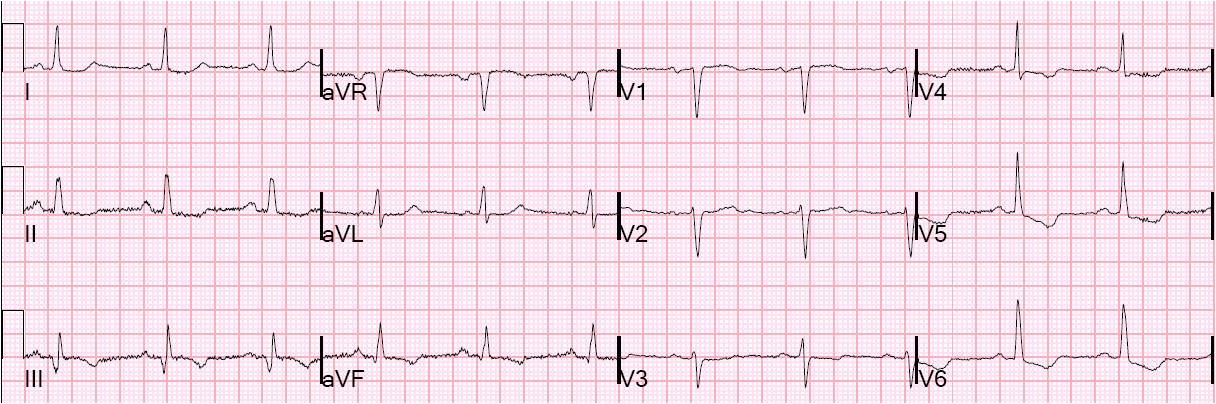
| There is 1 mm of ST elevation in V2 and V3, so this meets the criteria for reperfusion by the ACC/AHA guidelines. Unfortunately, the majority of patients who meet such “criteria” do not have MI. The most common reason for ST elevation is early repolarization. |
This could be early repolarization or acute anterior STEMI. How do we tell the difference?
A followup ECG and the answer is below.
In this case, the limb leads are suggestive of ischemia, with
some subtle ST depression inferiorly, suggesting pending ST elevation in
aVL due to lateral MI from proximal LAD occlusion.
If we apply the early repol vs. acute MI rule [see excel spreadsheet down the right side of the blog, which uses the formula (1.196 x STE at 60 ms after the J-point in V3 in mm) + (0.059 x computerized QTc) – (0.326 x R-wave Amplitude in V4 in mm)], and enter these values: STE at 60 ms after the J-point is 3.0 mm, QTc is 420 ms, and R-wave amplitude in V4 is 1.5 mm), then we get a result of 27.9 (it is anterior STEMI if the value is greater than 23.4).
A simple rule is the R-wave rule, which depends on the fact that, in BER, the R-wave is always well developed: If the mean R-wave amplitude from V2-V4 is less than 5 mm, then it is
almost certainly MI. If greater than 5 mm, it is probably BER. A cutoff
of 5 mm gives a sensitivity for MI of about 70%, but a specificity of
greater than 95%. This ECG has very poor R-wave progression and so it cannot be early repolarization.
The rule relies on the findings that the mean ST elevation was higher in the
MI group, and the mean QTc in BER is shorter (mean = 390 ms vs. 426 ms), and mean
R-wave amplitude is greater.
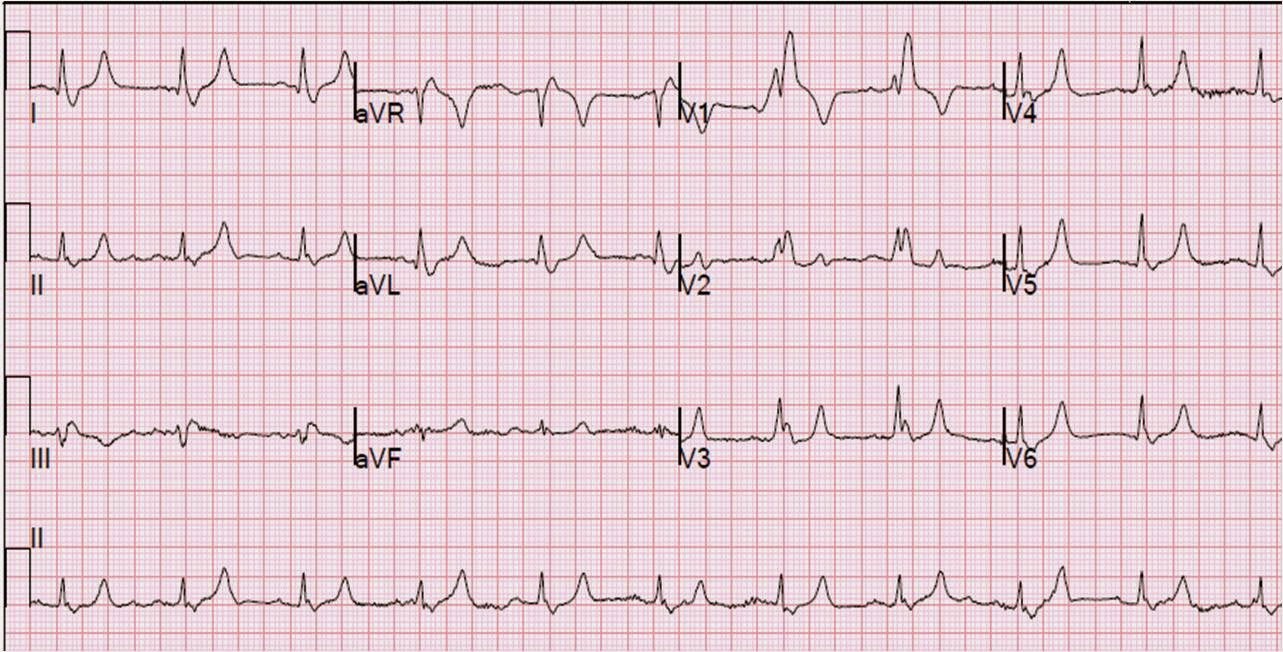
The clinicians were suspicious of MI, so they were smart to obtain serial ECGs. They obtained the second ECG at 0143:
 This shows unequivocal straightening of the ST segments, compared to the first ECG. This ST straightening results in T waves which are fattened and “hyperacute”. This is diagnostic of anterior STEMI.
This shows unequivocal straightening of the ST segments, compared to the first ECG. This ST straightening results in T waves which are fattened and “hyperacute”. This is diagnostic of anterior STEMI.
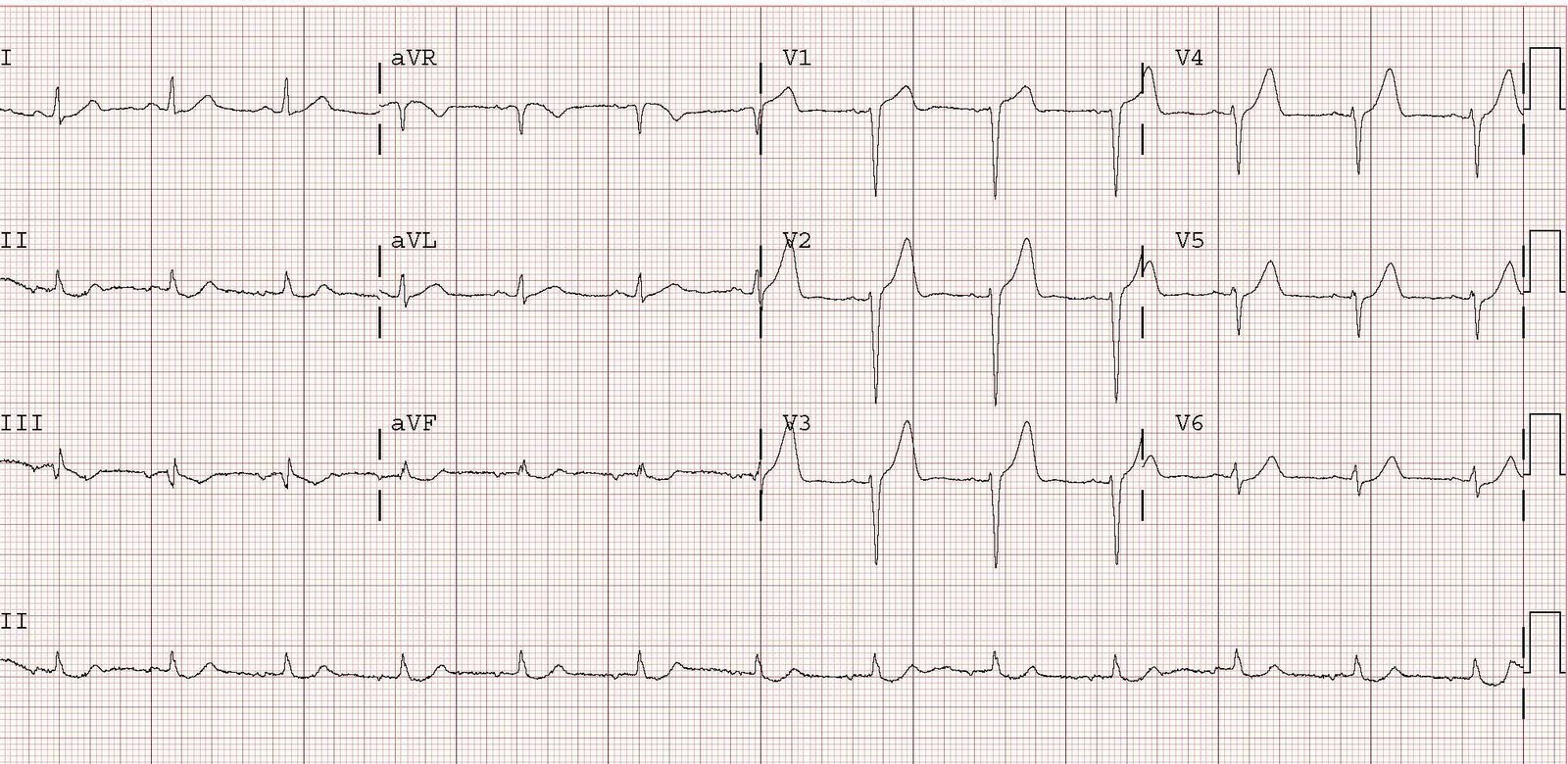
In case you can’t see this difference in the straightening of the ST segment, here they are side-by-side:

The diagnosis was not made until more ECGs were recorded, so reperfusion was slightly delayed. He had a 100% proximal thrombotic LAD occlusion with TIMI-0 flow. It was opened and stented. The peak troponin was 138 ng/ml, so this was a large AMI.