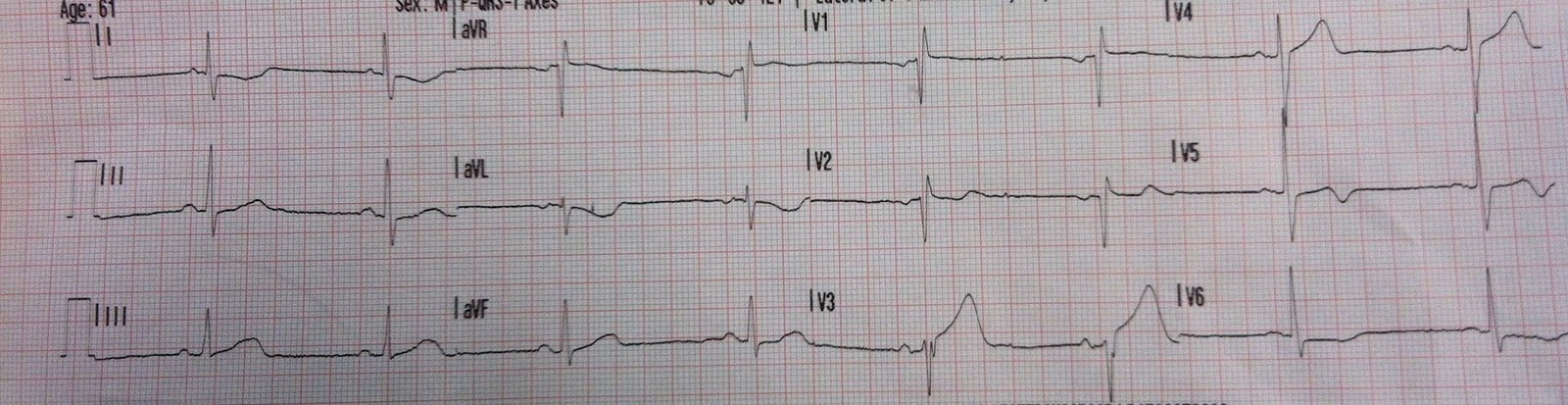
A middle-age alcoholic presents with weakness and vague abdomimal discomfort. The patient’s previous ECG was from 4 years prior and was completely normal. Here is the presenting ECG:
 |
| There is sinus rhythm and Right Bundle Branch block. There is a tall R-wave in V2 and V3 and slightly excessive ST depression in lead V2, with a biphasic wave. What is it? Is this ischemia? Is it posterior STEMI? Answer below. |
Answer:
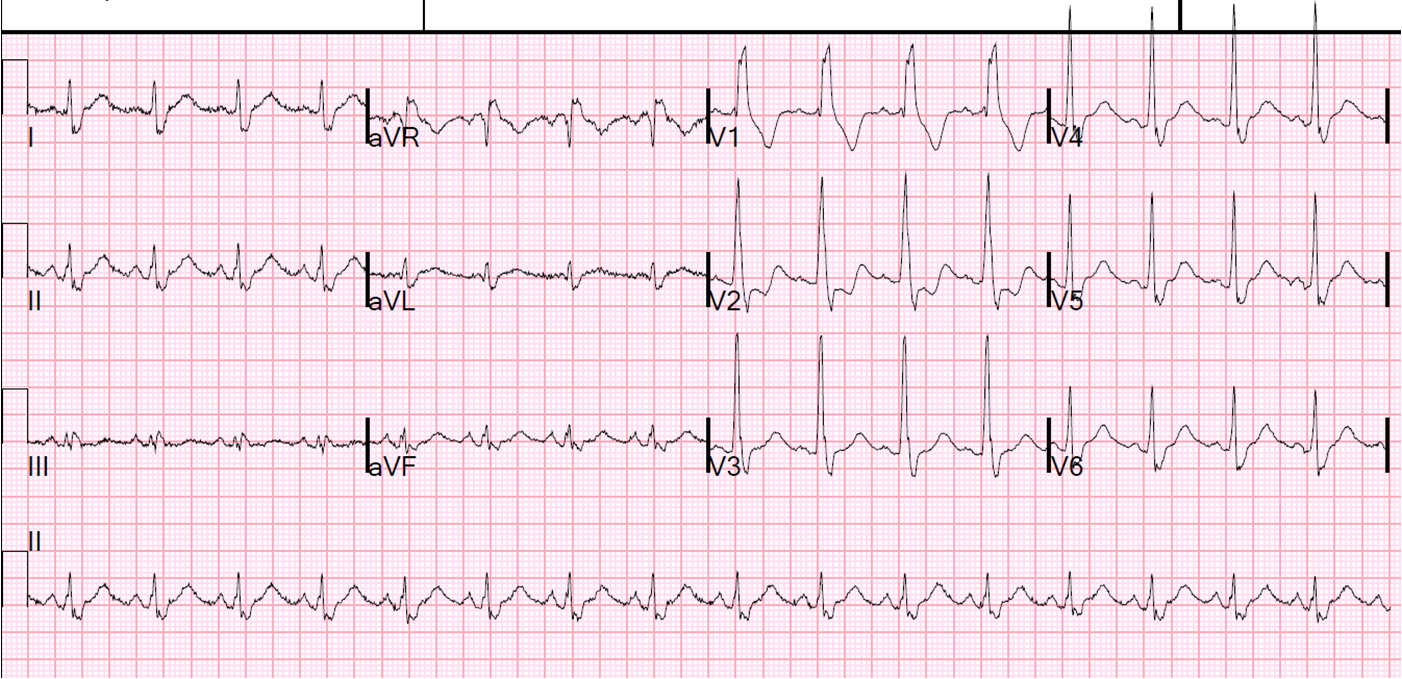
Here I have annotated the ECG:
 |
| The apex of the T-wave is seen in V1 (inverted). If you draw a line down to V2, you see that the nadir of the negative wave is at the same time as the peak of the T-wave in V1. The positive wave comes later. So this positive wave is a U-wave, not a biphasic T-wave. The arrow in V5 shows a small hump that is also U-wave. |
If the U-wave were really a T-wave, then the QT would be 440ms and the QTc would be 568 ms, which is very long. Whenever the QT interval seems too long, suspect a U-wave.
The patient had no myocardial ischemia. The potassium returned at 2.2 mEq/L.
Diagnosis: U-wave from hypokalemia, in the presence of right bundle branch block.