 |
|
|
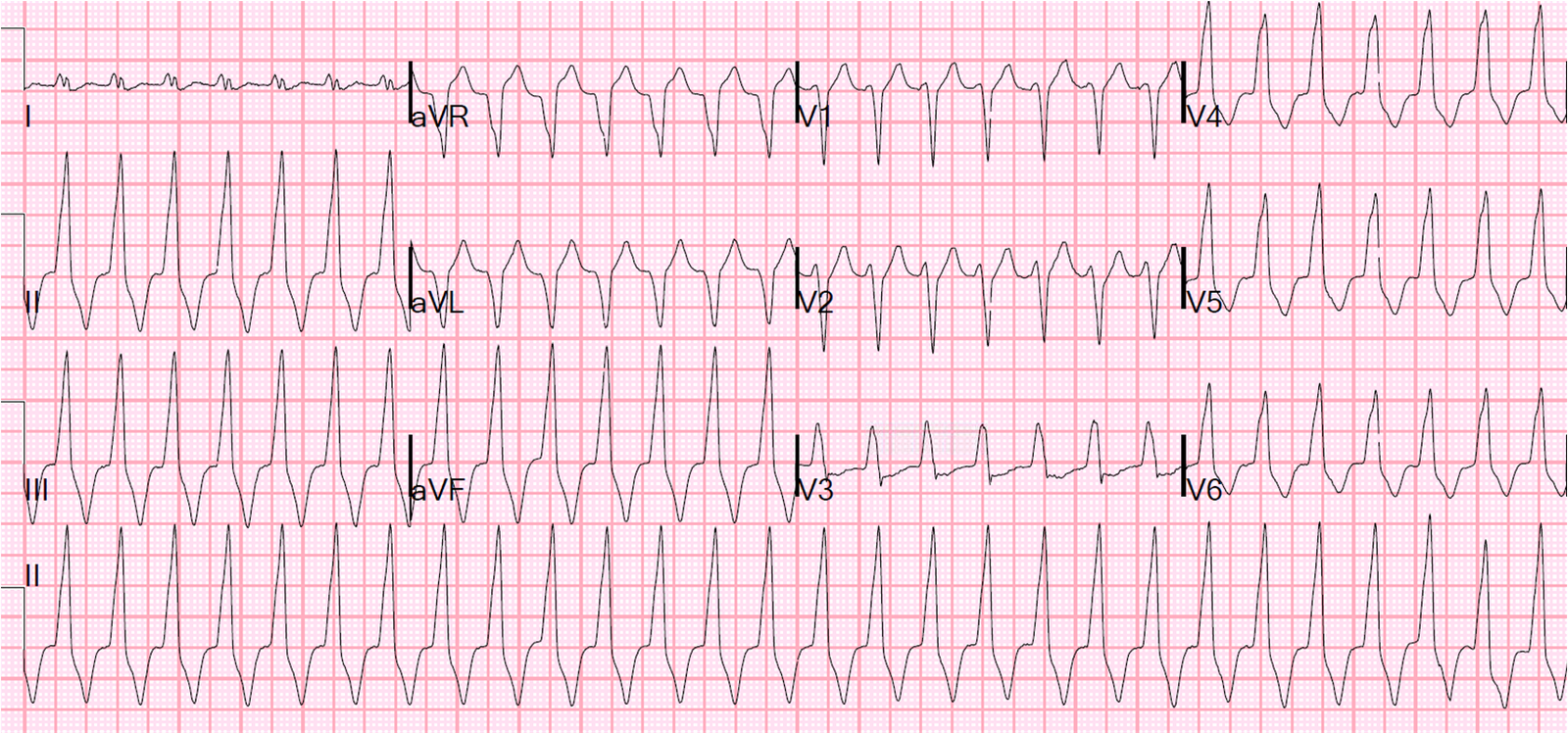
This is a classic pseudoinfarction pattern — hyperkalemia, with K of 6.9 due to DKA (pH 7.12, bicarb 6). In this case the diagnosis was easy because the patient presented very ill with known Type I diabetes and with vomiting, not chest pain.
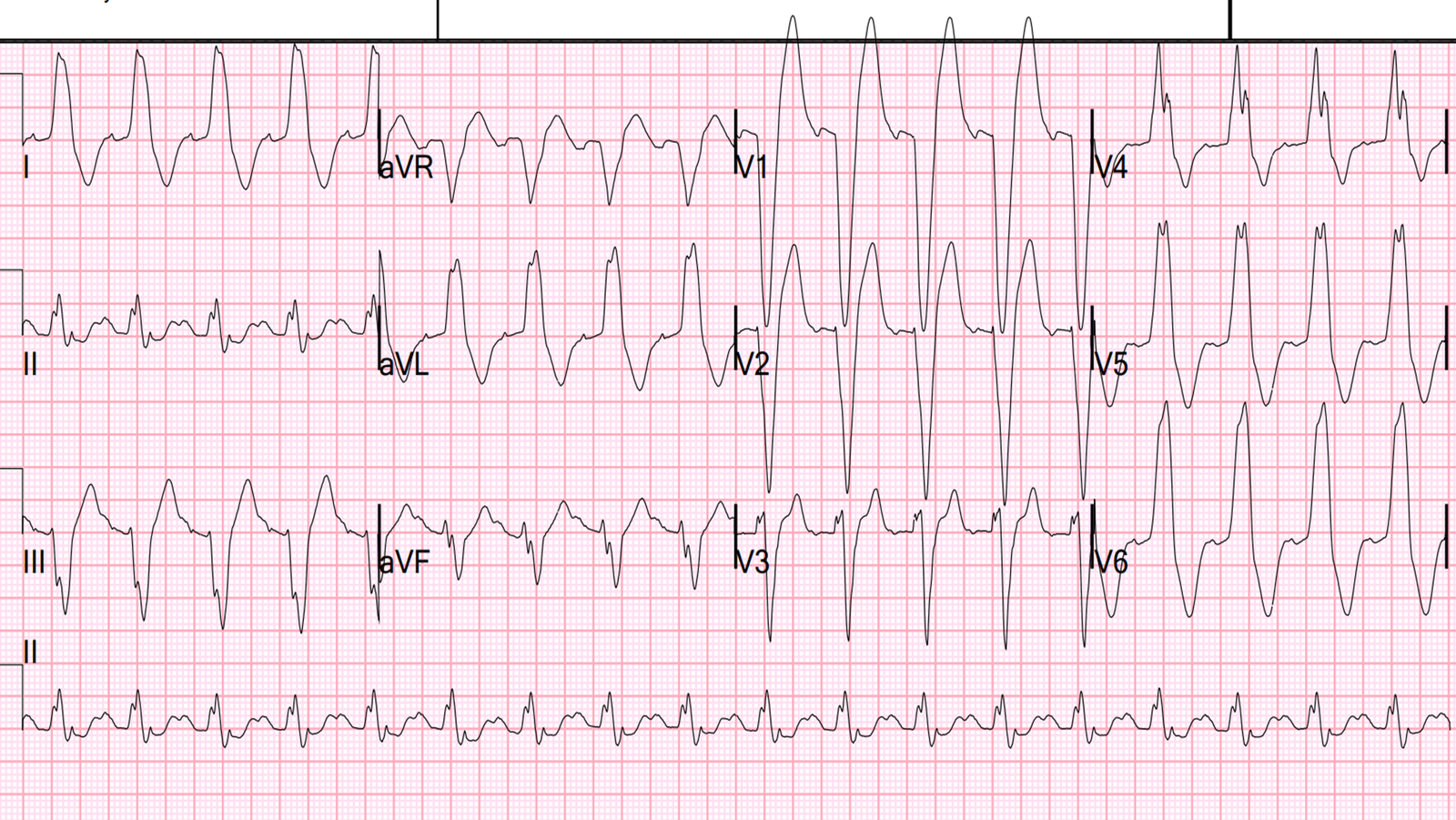
However, here are two from my files that presented with chest pain:
 |
| The peaked T-waves give it away, but the ST elevation in V1 and V2 is a little known pseudoinfarction pattern. There was no MI here. |
 |
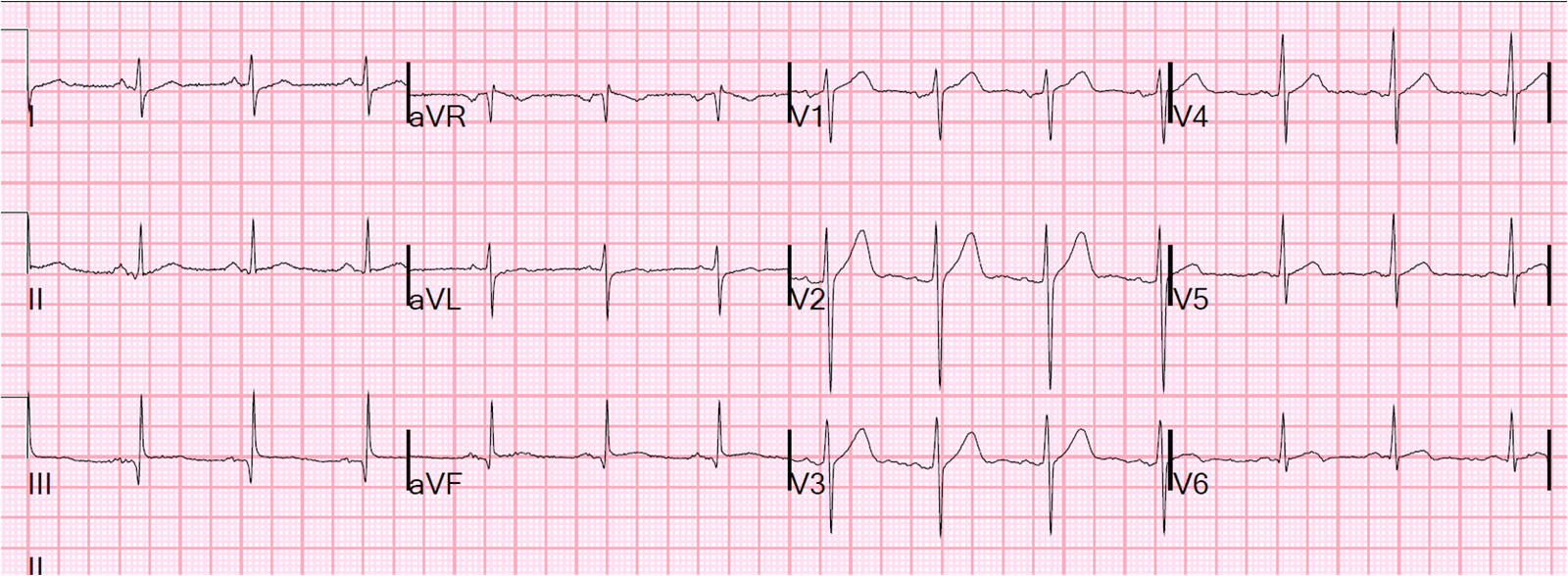
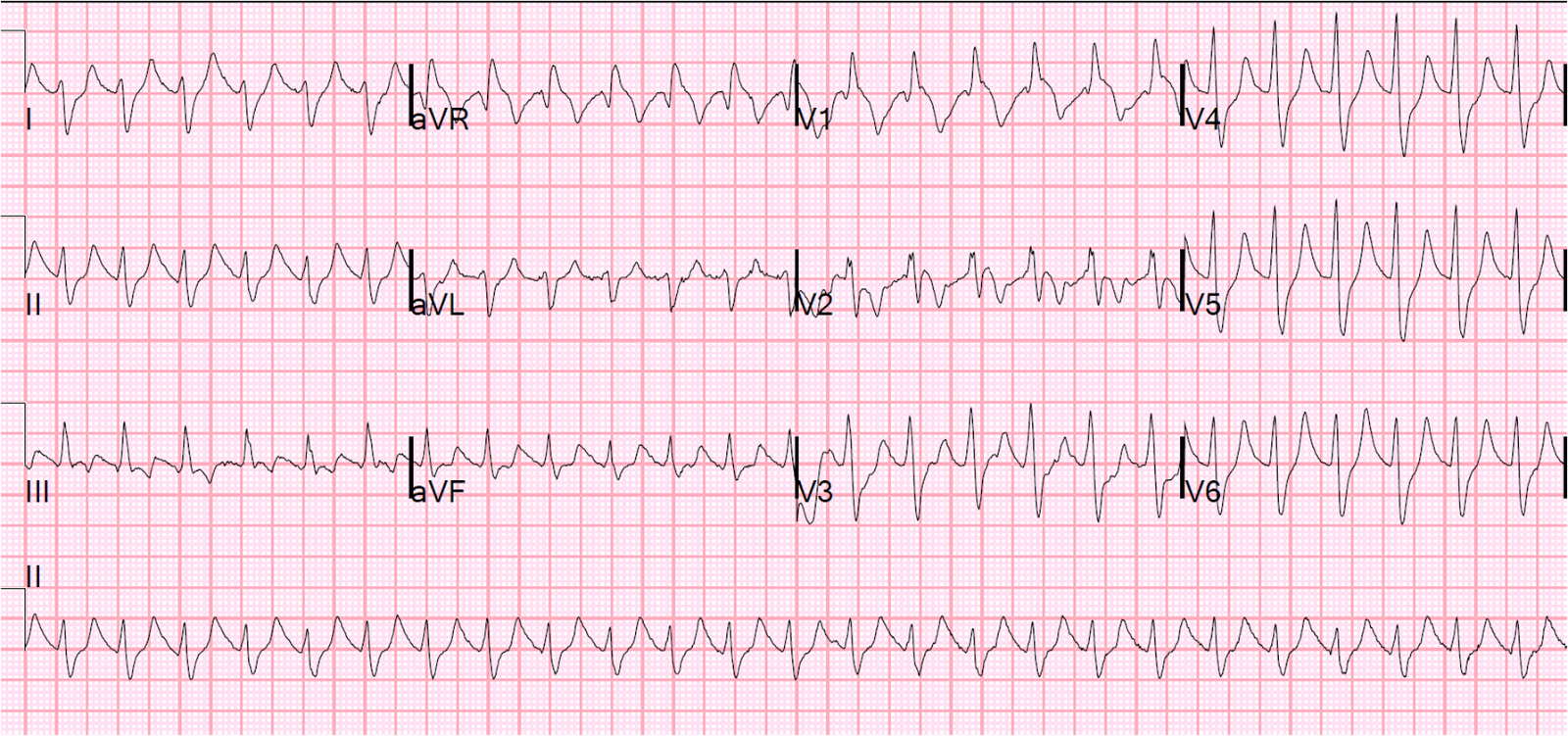
| Thanks to K. Wang for this EKG. Again, there was no MI, only hyperkalemia. |
In all 3 of these cases, the findings disappeared with treatment of hyperkalemia, and the ECG normalized.