This is a video I made a while back. I thought it was worth a re-post. For those who don’t have time to watch a video, you’ll have to read the ECG as shown on this still frame because I lost it and cannot post it.
See down below for explanation if you don’t want to watch the video.
See video here:
RV MI diagnosed by ST elevation in V1 from HQMedEd on Vimeo.
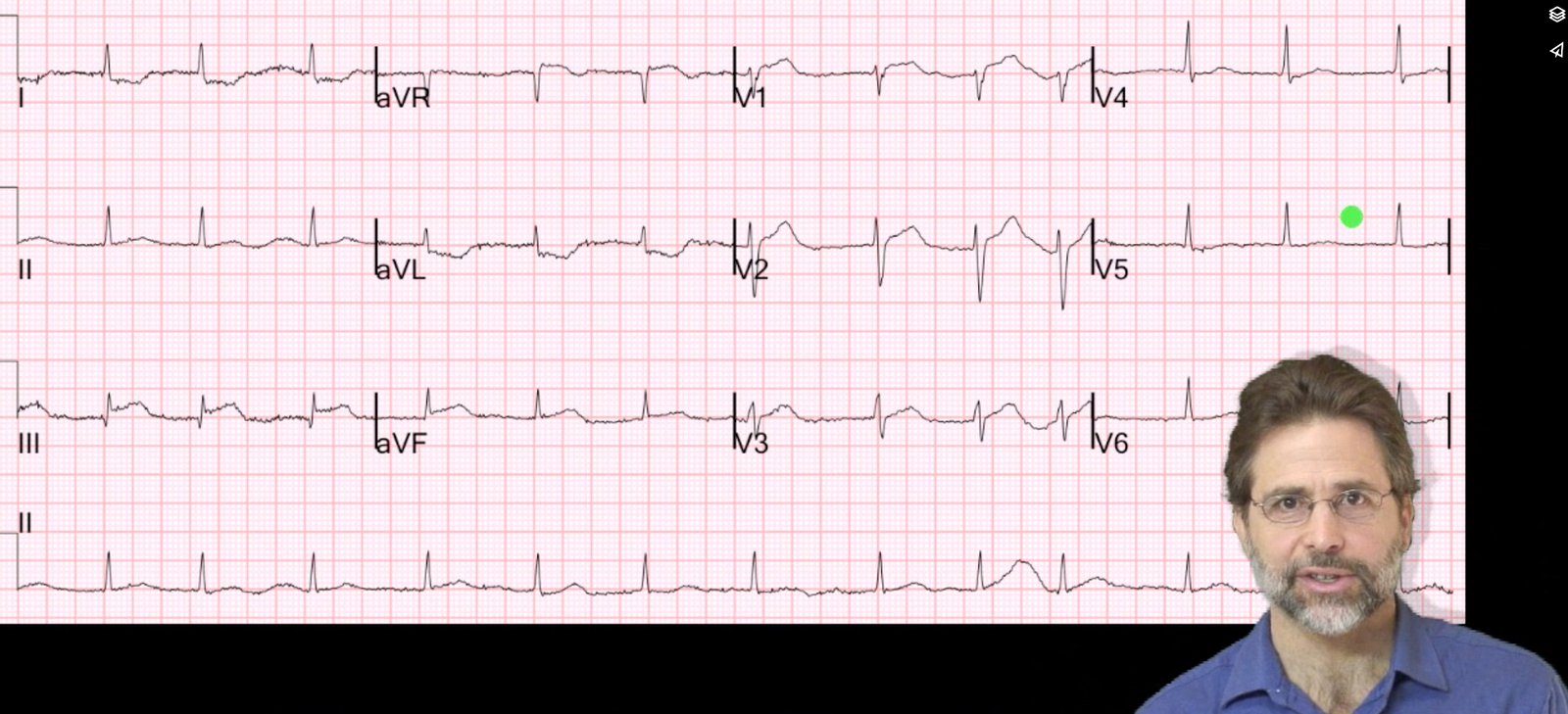
There is inferior STEMI. But there is also ST elevation in leads V1 and V2. When you see this, think right ventricular (RV) MI. The hypotension is further evidence for RV MI. There was no right sided ECG.
I heard about the case, and saw the ECG, shortly after the patient left for the cath lab. I called the interventionalist while the patient was on the table and he told me that the occlusion was not in the proximal RCA, but further down. I asked if he was sure about this, because the ECG would indicate a proximal RCA occlusion with RV MI. He took another look and realized that the culprit was indeed in the proximal RCA and that the thrombus had embolized distally. And so he put the stent in the proximal RCA.
Learning point: Even when you have an angiogram, the ECG findings make a difference.
A 56 year old woman with chest pain and hypotension: