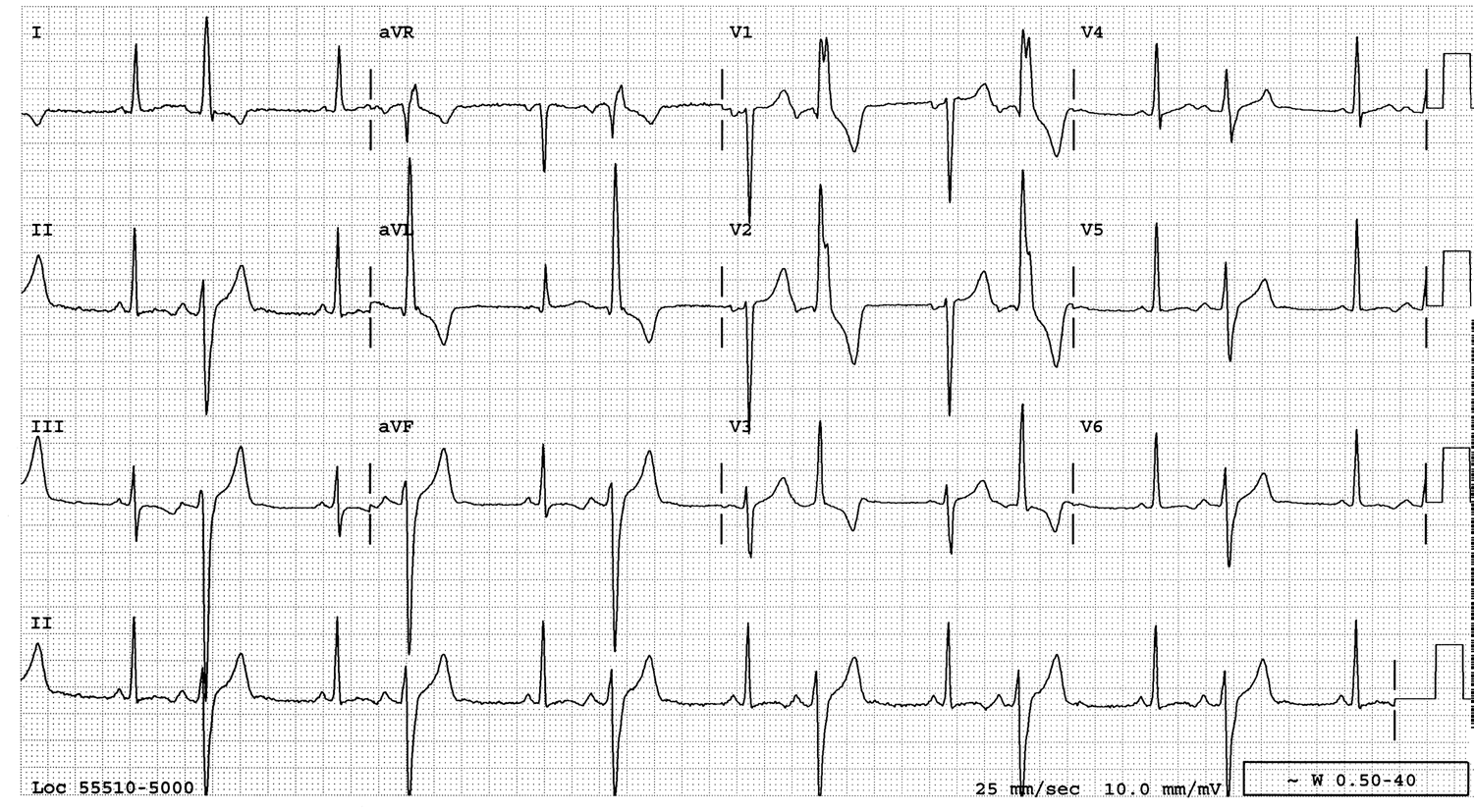
Medics recorded this ECG at time 0 in a patient with chest pain:
 |
| There are inferior hyperacute T-waves, with reciprocally inverted hyperacute T-wave in aVL, and a biphasic (down-up) T-wave in V2 and V3, as well as ST depression in I and V4-V6. |
“Down-up” biphasic T-waves should always be thought to be reciprocal of “up-down” (Wellens’ type) reperfusion T-waves. (Alternatively, if you see a down-up T-wave, it may actually be a down T-wave followed by an upright U-wave, if it happens very late.) Thus, this is probably inferior-posterior STEMI, possibly with some degree of reperfusion.
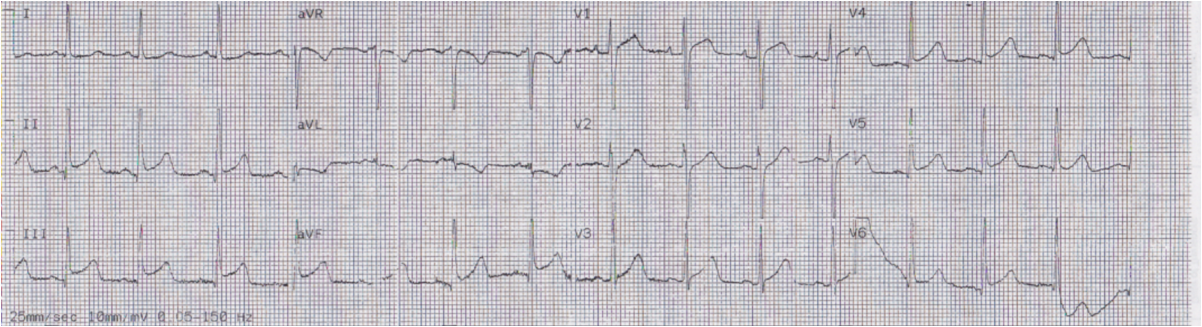
The chest pain began to resolve after NTG (t = 2 minutes):
 |
| Inferior T-waves are slightly smaller, and there is less negativity to the T-waves in V2 and V3 |
Another was recorded at t = 4 minutes:
 |
| Now inferior T-waves are not at all hyperacute and the precordial T-waves are mostly upright. Clearly, this is a reperfusing inferoposterior MI. There are down-up T-waves in V4-V6. |
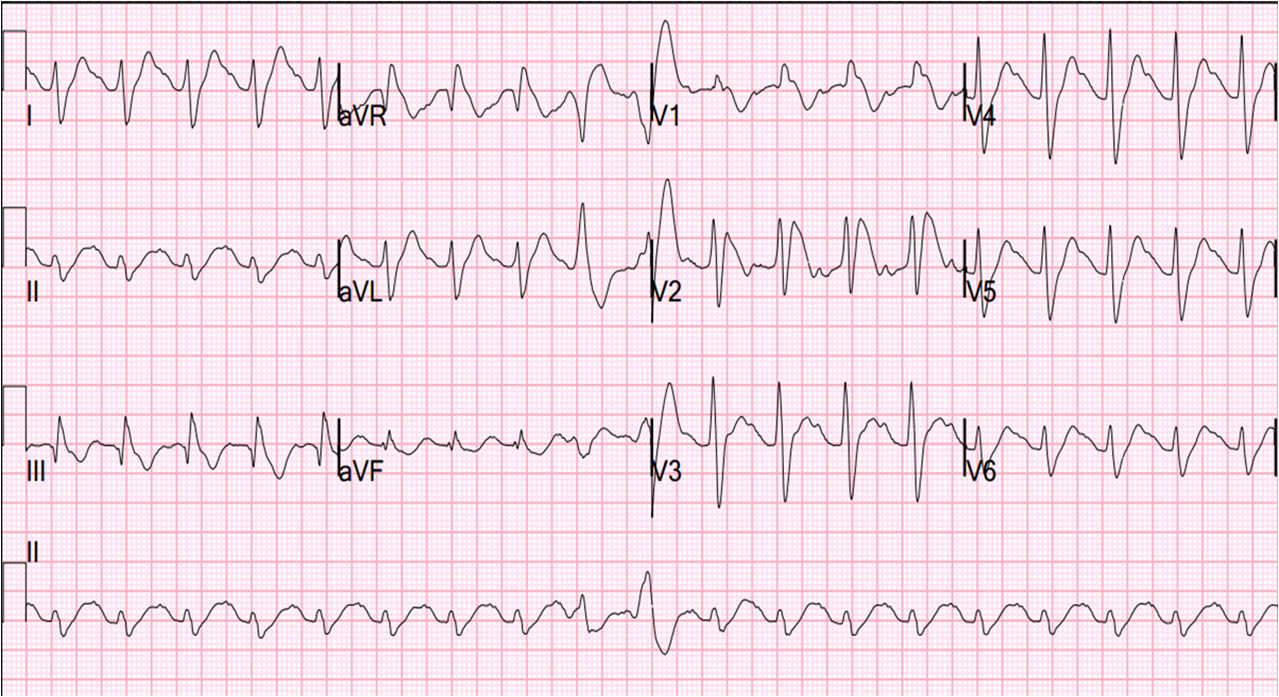
Here is t = 13 minutes, with posterior leads V7-V9:
 |
| Now there are inverted (reperfusion) T-waves in the inferior leads, with a reciprocally upright T-wave in aVL. The T-waves in V2 and V3 are upright. There are mostly inverted T-waves in V7-V9, pretty much reciprocal to (opposite of) V2 and V3. |
Here is t = 14 minutes (simultaneous to previous):
 |
| T-waves are upright in V4-V6, reciprocal to the inverted T-waves in V7-V9, but not exactly because these are not 180 degrees opposite each other. V2 and V3 are another example of posterior reperfusion T-waves. |
Angiogram showed an open culprit artery supplying the inferior and posterior walls