An 60-something man complained of sudden weakness. There was no chest pain or SOB. He had normal blood pressure and perfusion and was asymptomatic at rest. He was well appearing.
An ECG was recorded:
 |
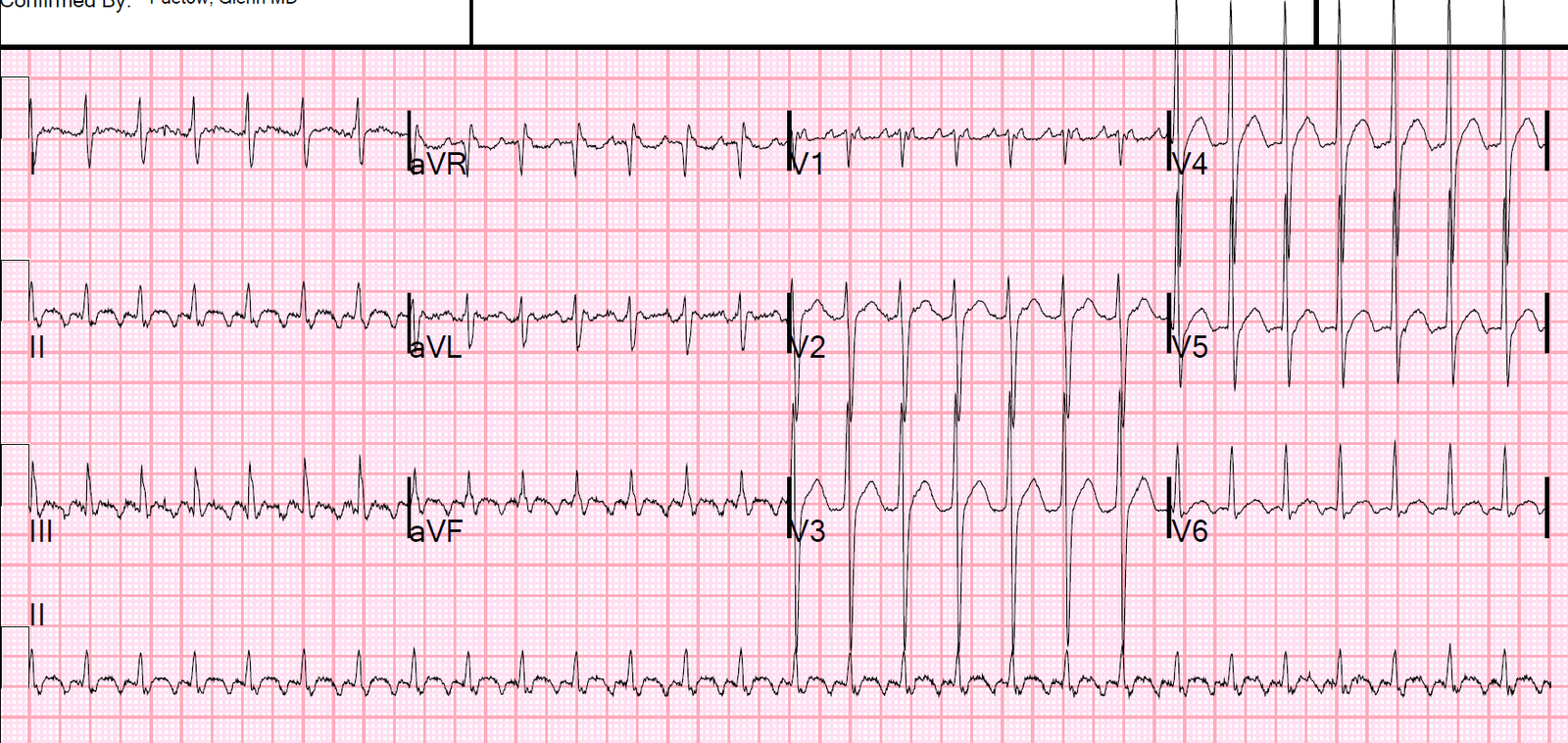
| There is a slow, wide rhythm with bizarre T-waves.What is it? What do you want to do? |
You’ll note there are P-waves.
Look at lead II across the bottom:
—There is a P-wave immediately after each T-wave (these do NOT conduct).
—There is a P-wave immediately before each QRS. Even though it appears as if that P-wave does not have enough time to conduct, the PR interval is exactly the same for every one of these, so it is very unlikely to be isorhythmic dissociation. Therefore, every other P-wave is conducting and it is thus 2nd degree AV block, Mobitz II.
Furthermore, there is a large R-wave in V1, with large S-wave in V5-V6 (RBBB) and also an axis toward aVR, implying a fascicular block as well.
We all know that there is a high incidence of progression from Mobitz II to third degree (complete) AV block, but we don’t always get to see it.
Such progression to complete heart block is especially likely when there is high degree block due to disease in the conducting fibers (in contrast to the AV node alone). And the fact that there is RBBB + fascicular block shows that there is disease in these conducting fibers also.
Here only one fascicle is working, and then it is only working on every other beat!!
Management: Since these patients are at high risk of progressing to complete heart block, especially in the context of acute MI (not applicable here), it is wise to apply the external pacing pads. Get ready for emergent transvenous pacing and get the patient to an electrophysiologist who can place a permanent pacemaker.
The electrophysiologist was called. The patient remained stable.
Electrolytes, especially K, were normal. Troponin was negative.
80 minutes later, we have this ECG:
 |
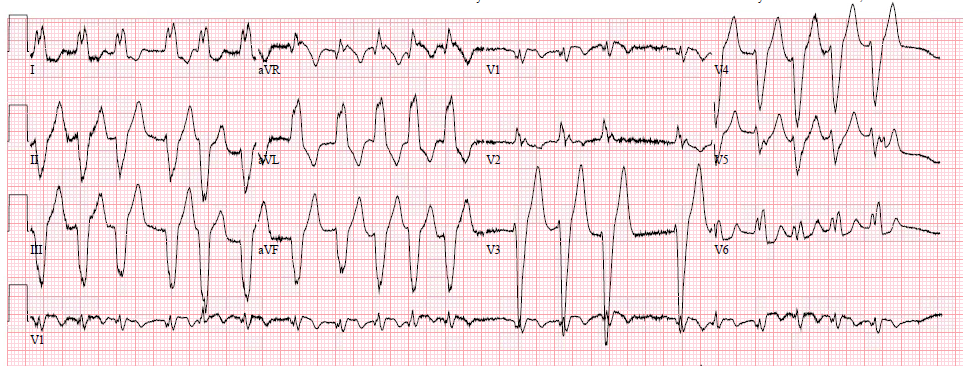
| Now what is going on? |
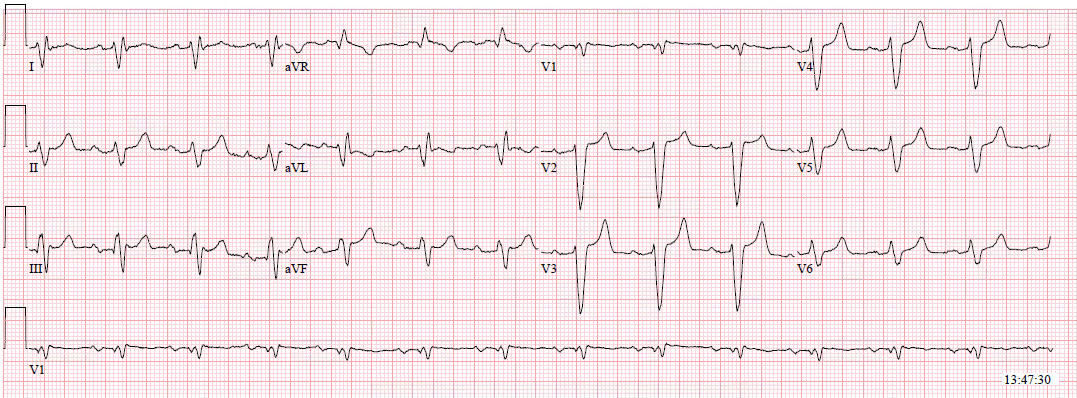
Here the ECG is annotated:
 |
| The black lines (lead II across the bottom) indicate the beginning of every P-wave.P-waves are at a rate of about 96. It appears that every other P-wave conducts [see complexes 1, 4, and 5 — not including the PVC (red arrow)] However, you can see that the P-waves encroach closer and closer to the QRS. The PR interval is getting shorter, if it is really a PR interval. Also, there are clearly P-waves that do NOT conduct. Thus, the P-waves that appear to conduct are only incidentally going approximately the same rate as the QRS and are not really conducting (isorhythmic dissociation) Furthermore, the QRS has changed from the first ECG: there is now more of a Left Bundle Branch Block pattern. This appears to be isorhythmic dissociation with third degree (complete) AV block. The QRS has changed because it has gone from a conducted beat to an escape beat.
Alternatively: this could be a junctional escape with alternating bundle branch block: formerly RBBB + fascicular block, now LBBB. The rate of 50 supports this. |
Isorhythmic dissociation:
P-waves are occurring at a rate of 96 and no P-wave is conducting. The ventricular escape is 50, which is slightly faster than half of the sinus rate (96 divided by 2 = 48). So every second P-wave occurs at about the same time as the ventricular escape (you have to ignore the PVC). But since the ventricular rate is slightly FASTER than half the sinus rate, it comes a bit earlier on each beat and therefore the PR interval appears to shorten. Really they are just coincidentally coming at almost the same time.
Most isorhythmic dissociation does not also have AV block. In this case, there is isorhythmic dissociation with complete AV block.
See this post on isorhythmic dissociation without block: What is this rhythm?
Clinical Course
Regardless of whether there was progression to complete heart block or not, the patient would need a pacemaker.
A pacemaker was implanted. There was no myocardial infarction. The etiology was not yet found.
How about those T-waves??
These are common in high grade AV block. You can read more about them here: