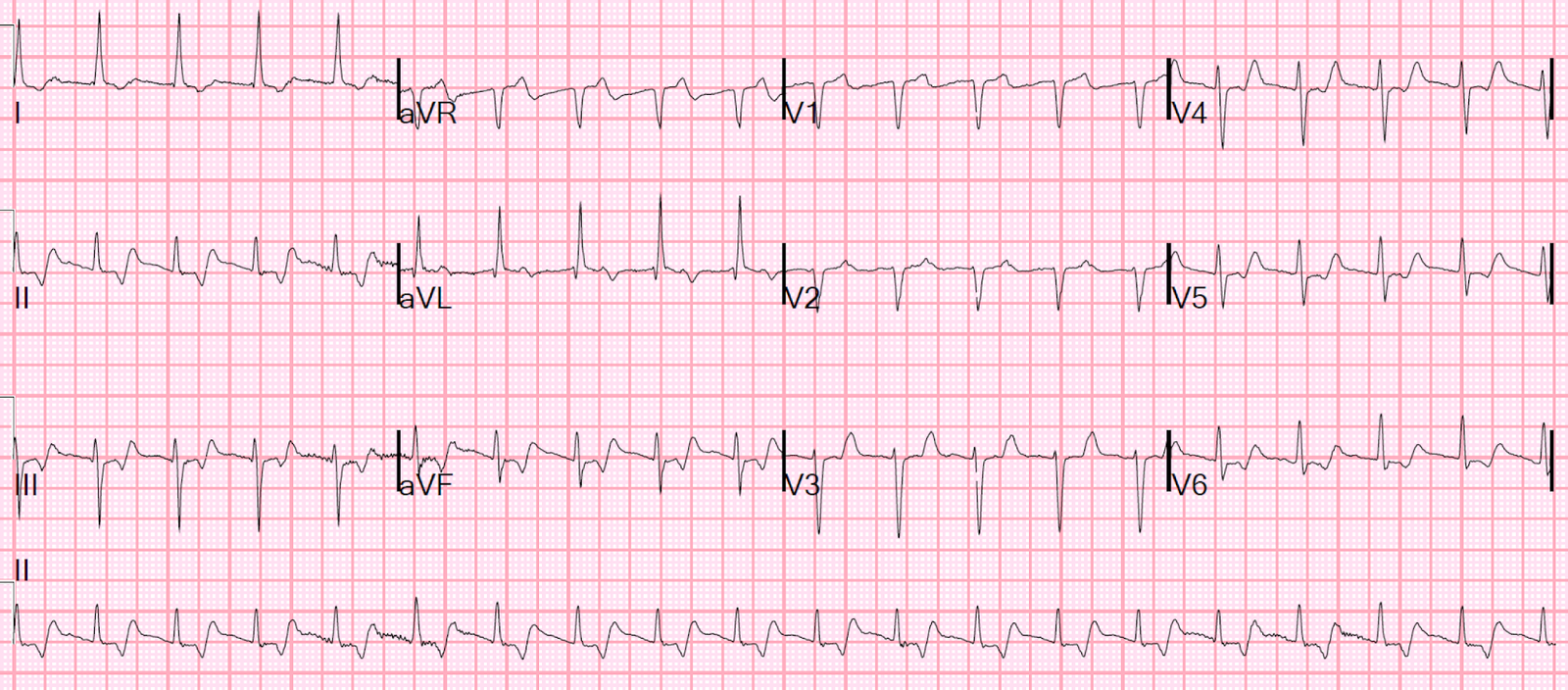
This ECG was sent along with this text:
“Thoughts? Occlusion or not? – context : cardiac arrest:”
 |
| Here is my answer:
“Yes, but probably > 6 hours old, or an acute superimposed on an old MI, but there is acute STEMI here.”
Question:
“You think the ST elevation is diagnostic according to criteria?”
Answer (Quoted):
“Not according to criteria. But you cannot call it normal variant ST elevation when there are Q-waves like that.”
So the differential is: “Old MI with persistent ST elevation (LV aneurysm)” vs. “Subacute MI” vs. “Old MI with superimposed STEMI.”
“I have derived and validated a formula to differentiate LV aneurysm from acute MI: if there is one lead of V1-V4 with a T/QRS ratio > 0.36, then it is 90% specific for acute. In this case, V3 has a 5 mm T-wave and the QRS amplitude is 8.5 mm. 5/8.5 = about 0.6 which is far higher than 0.36.” Also V4.
Question:
How about ultrasound?
Answer:
“There will be an anterior wall motion abnormality (WMA) for sure, but you won’t be able to tell whether it is old or old with superimposed acute. Either one could have WMA with thinned out wall. Only acute has a T-wave like that.”
Outcome:
“I pushed for the activation – proximal LAD 100% – I’m glad I pushed for it. First troponin I returned at 11.”
My answer:
“Just as I said: Subacute STEMI” |
Aside: Ryan Tee also noted correctly that there is also a PVC in aVL with concordant ST elevation. This is a very good sign for STEMI, but it could possibly also be seen in LV aneurysm.
Comment
One might say that any shockable cardiac arrest should go to the cath lab emergently, and there are many good arguments for that. Most of these arguments are based on “if there is no alternative explanation.”
Old MI is such an alternative explanation, as it supplies the underlying substrate (scarred myocardium) that leads to ventricular fibrillation.
Furthermore, not all hospitals actually take all shockable cardiac arrests for angiogram, but rather do so selectively for those with ECG evidence of ischemia (especially, of course, STEMI).
In this case there is a clear alternative diagnosis: old MI, and no obvious ischemia on the ECG.
But that is only true if you do not understand the T-wave in old MI: it is not large, but rather small or slightly inverted.
The T-waves were too large and upright in V3 and V4 to be due to old MI. They had to be acute (or, I should say, subacute). This is confirmed by the initial troponin of 11, which is only present in MI that has been going on for “a while” (at least 6 hours).
Brooks Walsh recently wrote this post which explains it all in much more detail.