A 60 yo woman presented with CP and troponin I of 0.85 ng/ml.
 |
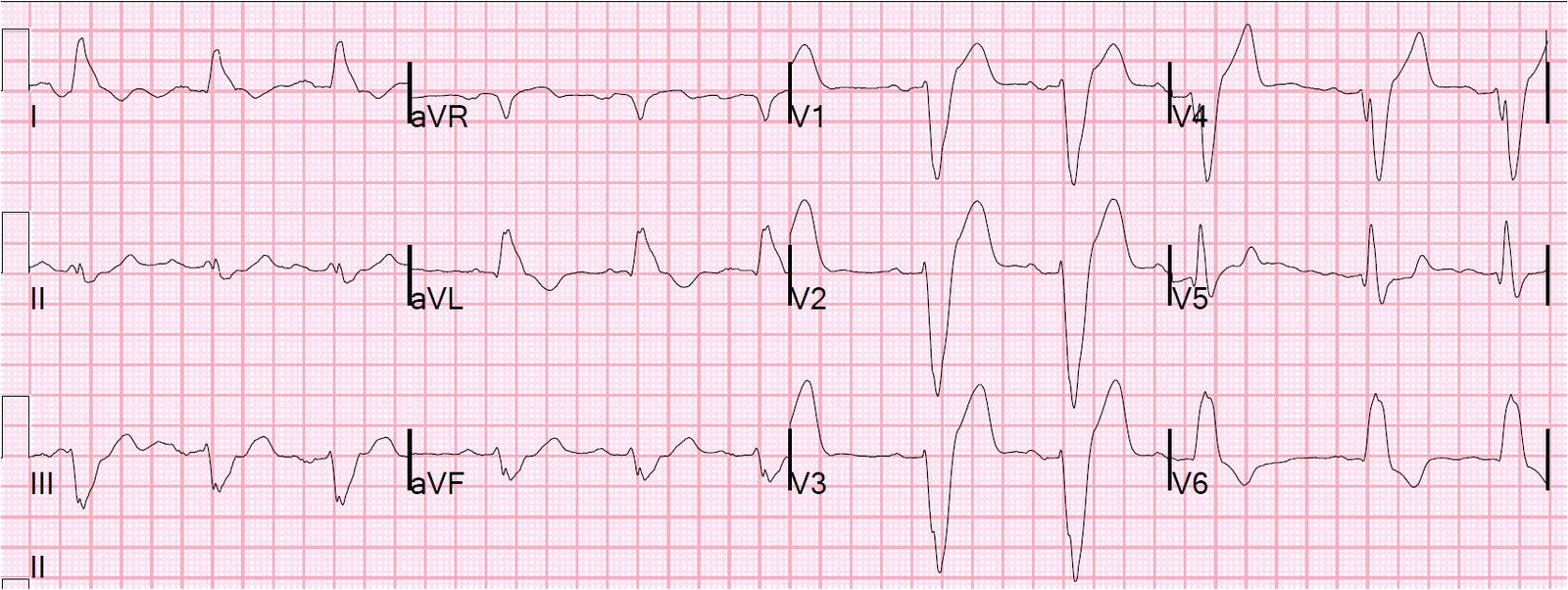
| There is RBBB, but without the usual rSR’ in right precordial leads. [There is some left axis deviation as well, probably a left anterior fascicular (hemi-) block.] The initial r-wave is gone, so that there are QR-waves (diagnostic of myocardial infarction, whether old or acute). There is ST elevation (which is never normal in RBBB). The negative T-wave makes it very unlikely that this acute MI, but it could be either subacute or old. |
My interpretation was RBBB with old anterior MI and LV aneurysm. We admitted her treated her for NonSTEMI.
Subsequent course:
There was no ECG evolution. Echo showed decreased left ventricular systolic performance, at least moderate, with an estimated EF = 35 – 40%. There was a regional wall motion abnormality in the LAD distribution: distal septum, anterior and apex, large and the wall was “akinetic or possibly dyskinetic,” confirming LV aneurysm. There was also a left ventricular apical thrombus, which is a frequent complication of aneurysms.
She was treated medically for her NonSTEMI and LV thrombus.
Here is a very detailed discussion of RBBB with LV aneurysm, with several ECGs.